

The correlation between raised body mass index and assisted reproductive treatment outcomes: a systematic review and meta-analysis of the evidence
- PMID: 29486787
- PMCID: PMC5830337
- DOI: 10.1186/s12978-018-0481-z
The correlation between raised body mass index and assisted reproductive treatment outcomes: a systematic review and meta-analysis of the evidence
Abstract
Background: Public funding for fertility services within the United Kingdom is limited, and therefore, strict guidance exists regarding who can be offered treatment under the National Health Service (NHS). Body mass index (BMI) is a universal criteria adopted by both the public and private sector. This study addresses an important aspect of the impact of a raised BMI on fertility treatment outcomes. We standardise the analysis of the data by only including studies incorporating the WHO BMI criteria; the current reference point for clinicians and clinical commissioning groups in ascertaining which group of patients should receive treatment. This study is an update of the previous systematic review performed in 2010, with the inclusion of a larger number of cycles from central databases such as the Society for Assisted Reproductive Technology (SART).
Methods: An electronic literature search was conducted through the Cochrane, Medline and Embase libraries. Data extraction for each outcome measure was pooled and expressed as an odds ratio with 95% confidence intervals. Where clinical heterogeneity was evident, the random effects model was used to calculate the risk ratio and a fixed effects model was used for the remaining studies. A p value < 0.05 was considered statistically significant.
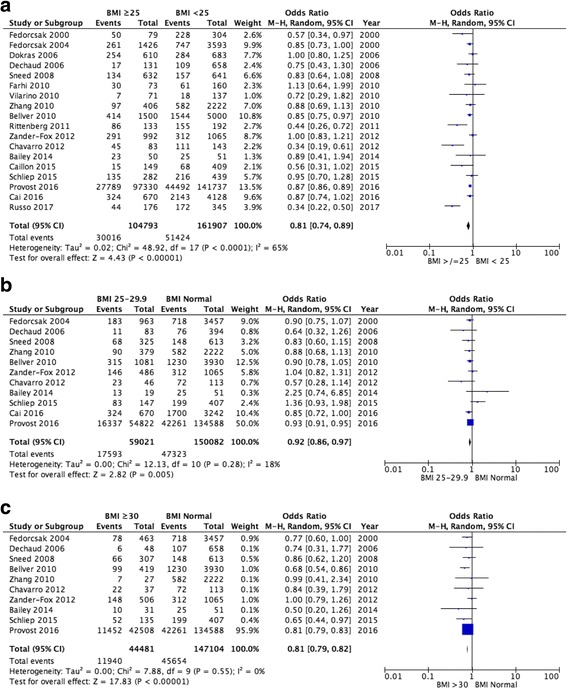
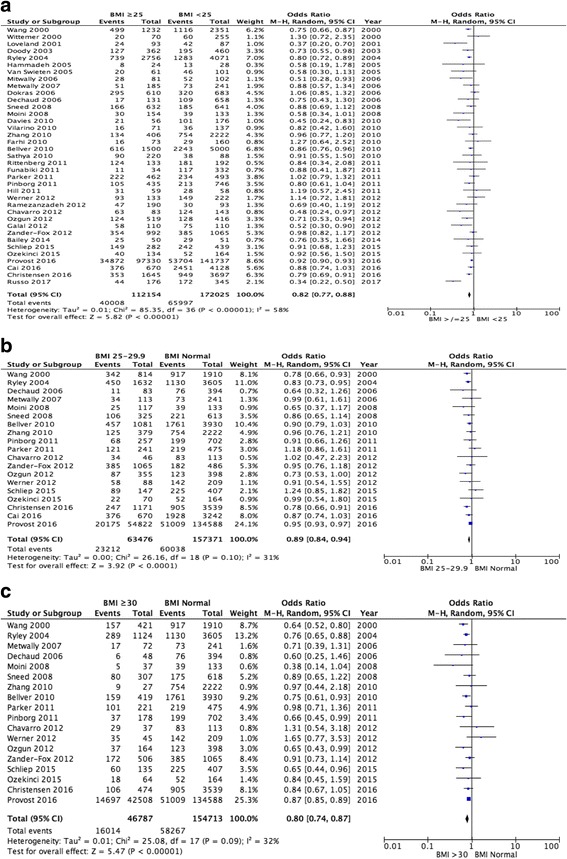
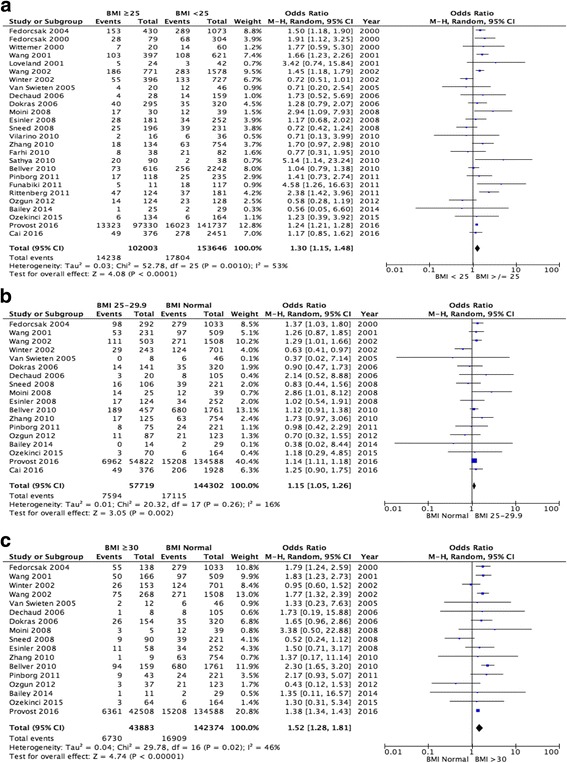
Results: A total of 49 studies have been identified and included in this systematic review. Overweight and obese (BMI ≥ 25 kg/m2) women have a statistically significant lower live birth rate (OR 0.81, 95% CI 0.74-0.89, p < 0.00001) following Assisted Reproductive Technology (ART) when comparisons are drawn to women with a normal BMI. An increase is also demonstrated in the number of miscarriages experienced by women with a BMI ≥ 30 kg/m2 (OR 1.52, 95% CI 1.28-1.81, p < 0.00001).
Conclusion: Although this review concludes that a clear impact of BMI on ART outcomes is demonstrated, there remains questions as to the pathophysiology underlying these differences. This review supports the government's stringent criteria regarding BMI categories under which NHS funding is made available for ART, through a clear description of poor reproductive outcomes in women with a BMI ≥ 30 kg/m2.
Keywords: Assisted reproductive technology (ART); Body mass index (BMI); Obese; Overweight.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- WHO. Obesity and overweight. Geneva: World Health Organization. Fact Sheet 311. Available from http://www.who.int/mediacentre/factsheets/fs311/en/.
-
- Mantel N, Haenszel W. Statistical aspects of the analysis of data from retrospective studies of disease. J Natl Cancer Inst. 1959;22:719–748. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
