

Second-Line Treatment Landscape for Renal Cell Carcinoma: A Comprehensive Review
- PMID: 29487224
- PMCID: PMC5947457
- DOI: 10.1634/theoncologist.2017-0534
Second-Line Treatment Landscape for Renal Cell Carcinoma: A Comprehensive Review
Abstract
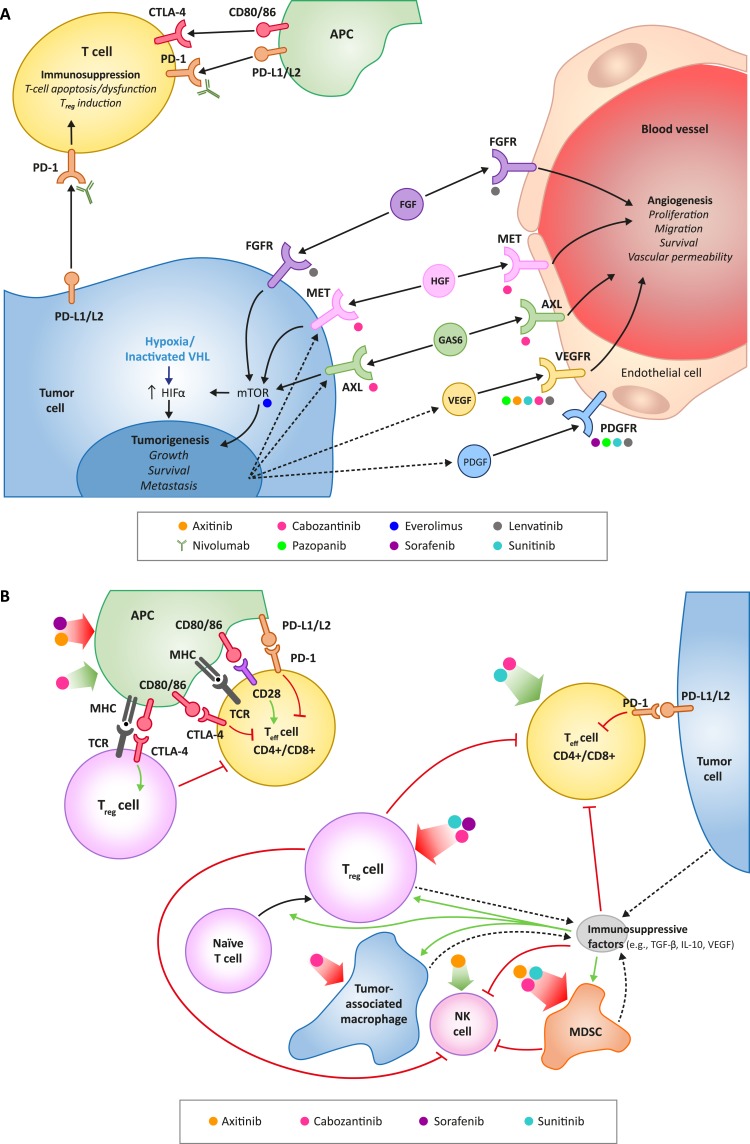
The management of advanced clear-cell renal cell carcinoma has steadily improved over the past decade with the introduction of antiangiogenic and targeted therapies. Recently, three new therapies have been approved for use as second-line options that further advance the treatment armamentarium: nivolumab, a monoclonal antibody targeting the programmed cell death receptor; cabozantinib, a small-molecule tyrosine kinase inhibitor (TKI) of vascular endothelial growth factor receptor (VEGFR), MET, and AXL; and lenvatinib, a small-molecule TKI of VEGF and fibroblast growth factor receptors that is used in combination with everolimus, an inhibitor of the mechanistic target of rapamycin. Together, these and previously approved second-line treatments offer clinicians the ability to better individualize treatment for patients after progression on first-line VEGFR-targeted therapies. In this comprehensive review, we discuss the efficacy and safety results from the pivotal trials of these newly approved therapies, including the quality of study design, the level of evidence, subgroup analyses, and how these data can help to guide clinicians to select the most appropriate second-line therapy for their patients.
Implications for practice: This review article provides the reader with a comprehensive overview of current treatment options for patients with advanced clear-cell renal cell carcinoma (RCC) whose disease has progressed after their first therapy. As many patients with RCC experience disease progression with initial treatments, effective second-line therapies are critical. Nivolumab, cabozantinib, and lenvatinib plus everolimus have recently been approved as second-line treatments. The new agents discussed in this review increase the therapeutic options available and provide physicians with opportunities to individualize treatments for their patients, with a view to improving disease control and survival outcomes.
Keywords: Axitinib; Cabozantinib; Everolimus; Lenvatinib; Nivolumab; Renal cell carcinoma.
© AlphaMed Press 2018.
Conflict of interest statement
Disclosures of potential conflicts of interest may be found at the end of this article.
Figures
References
-
- National Comprehensive Cancer Network. NCCN Guidelines: Kidney Cancer. Version 2.2017. Available at https://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf. Accessed November 2, 2016.
-
- Surveillance, Epidemiology, and End Results Program, National Cancer Institute. Cancer stat facts: Kidney and renal pelvis cancer. Available at https://seer.cancer.gov/statfacts/html/kidrp.html. Accessed March 28, 2017.
-
- Cindolo L, Patard JJ, Chiodini P et al. Comparison of predictive accuracy of four prognostic models for nonmetastatic renal cell carcinoma after nephrectomy: A multicenter European study. Cancer 2005;104:1362–1371. - PubMed
-
- Sorbellini M, Kattan MW, Snyder ME et al. A postoperative prognostic nomogram predicting recurrence for patients with conventional clear cell renal cell carcinoma. J Urol 2005;173:48–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
