

Ketamine has distinct electrophysiological and behavioral effects in depressed and healthy subjects
- PMID: 29487402
- PMCID: PMC6111001
- DOI: 10.1038/s41380-018-0028-2
Ketamine has distinct electrophysiological and behavioral effects in depressed and healthy subjects
Abstract
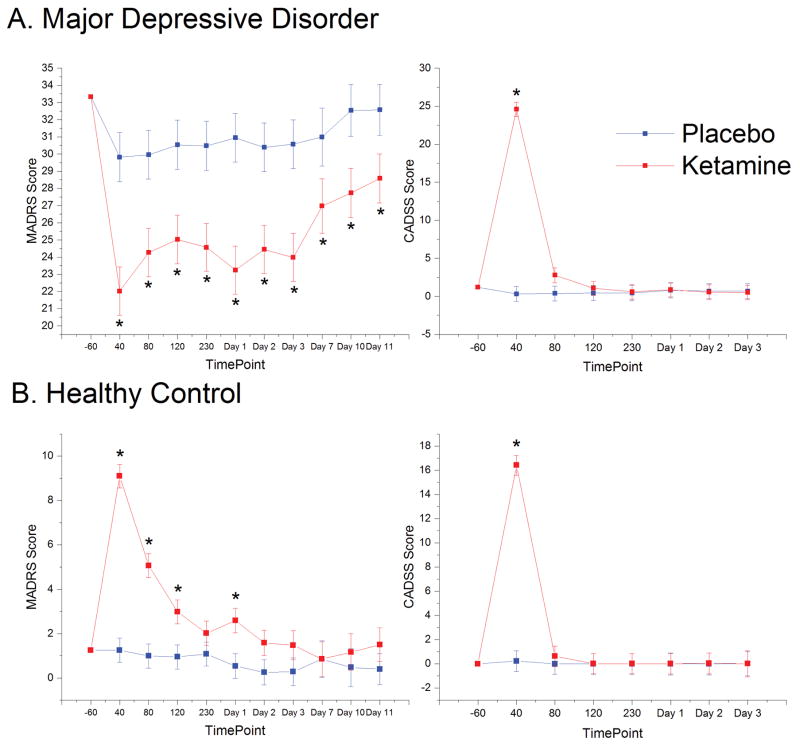
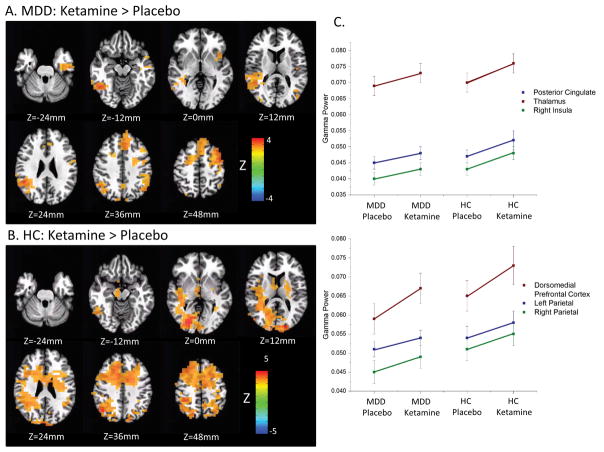
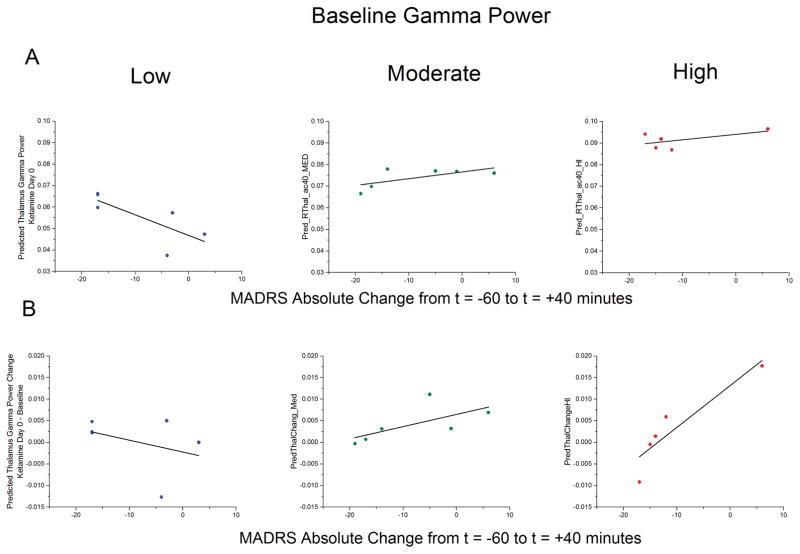
Ketamine's mechanism of action was assessed using gamma power from magnetoencephalography (MEG) as a proxy measure for homeostatic balance in 35 unmedicated subjects with major depressive disorder (MDD) and 25 healthy controls enrolled in a double-blind, placebo-controlled, randomized cross-over trial of 0.5 mg/kg ketamine. MDD subjects showed significant improvements in depressive symptoms, and healthy control subjects exhibited modest but significant increases in depressive symptoms for up to 1 day after ketamine administration. Both groups showed increased resting gamma power following ketamine. In MDD subjects, gamma power was not associated with the magnitude of the antidepressant effect. However, baseline gamma power was found to moderate the relationship between post-ketamine gamma power and antidepressant response; specifically, higher post-ketamine gamma power was associated with better response in MDD subjects with lower baseline gamma, with an inverted relationship in MDD subjects with higher baseline gamma. This relationship was observed in multiple regions involved in networks hypothesized to be involved in the pathophysiology of MDD. This finding suggests biological subtypes based on the direction of homeostatic dysregulation and has important implications for inferring ketamine's mechanism of action from studies of healthy controls alone.
Conflict of interest statement
Funding for this work was supported by the Intramural Research Program at the National Institute of Mental Health, National Institutes of Health (IRP-NIMH-NIH; NCT00088699/04-M-0222/ZIA MH002857), by a NARSAD Independent Investigator Award to Dr. Zarate, and by a Brain and Behavior Mood Disorders Research Award to Dr. Zarate. Dr. Zarate is listed as a coinventor on a patent for the use of ketamine in major depression and suicidal ideation. Dr. Zarate is listed as a co-inventor on a patent for the use of (2
Figures
References
-
- Trivedi MH, Rush AJ, Wisniewski SR, Nierenberg AA, Warden D, Ritz L, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry. 2006 Jan;163:28–40. - PubMed
-
- Zarate CA, Jr, Singh JB, Carlson PJ, Brutsche NE, Ameli R, Luckenbaugh DA, et al. A randomized trial of an N-methyl-D-aspartate antagonist in treatment-resistant major depression. Arch Gen Psychiatry. 2006 Aug;63:856–864. - PubMed
-
- Singh JB, Fedgchin M, Daly EJ, De Boer P, Cooper K, Lim P, et al. A Double-Blind, Randomized, Placebo-Controlled, Dose-Frequency Study of Intravenous Ketamine in Patients With Treatment-Resistant Depression. Am J Psychiatry. 2016 Aug 01;173:816–826. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
