

From CD4-Based Initiation to Treating All HIV-Infected Adults Immediately: An Evidence-Based Meta-analysis
- PMID: 29487595
- PMCID: PMC5816781
- DOI: 10.3389/fimmu.2018.00212
From CD4-Based Initiation to Treating All HIV-Infected Adults Immediately: An Evidence-Based Meta-analysis
Abstract
Background: The World Health Organization (WHO) Consolidated antiretroviral therapy (ART) guidelines set the CD4+ T-cell counts threshold to 500 cells/mm3 in 2013, and 2015 guidelines recommend treating all HIV-infected adults regardless of their CD4+ T-cell counts. To inform the decision-making around ART guidelines for people living with HIV, we systematically reviewed the literature to estimate differences in clinical benefits between individuals starting treatment with baseline CD4+ T-cell counts ≥500 cells/mm3 (early initiation) as compared to <500 cells/mm3 (deferred initiation).
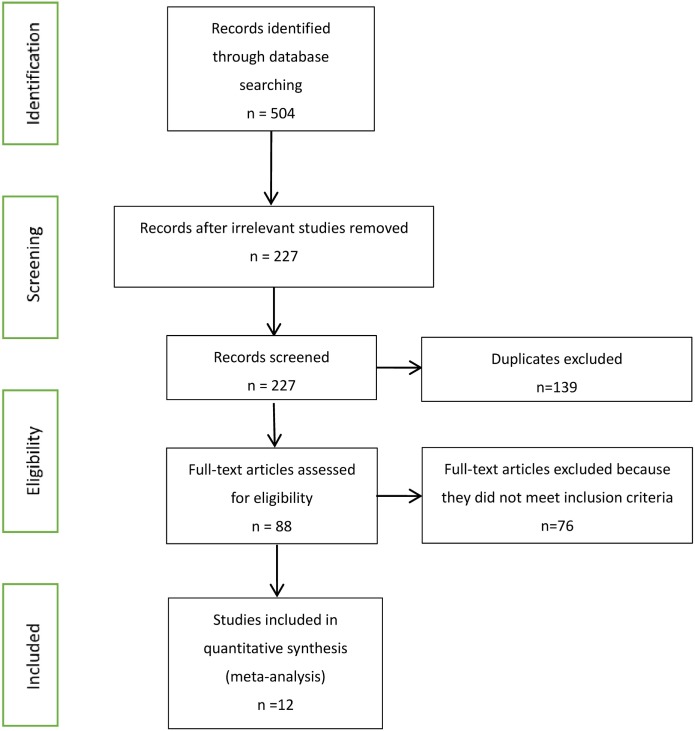
Methods: We systematically searched the electronic databases and abstracts for randomized controlled trials (RCT) and observational studies. Outcomes were mortality, AIDS progression, AIDS or death, immunologic recovery, and virologic suppression. We pooled data across studies and performed analyses of effect sizes.
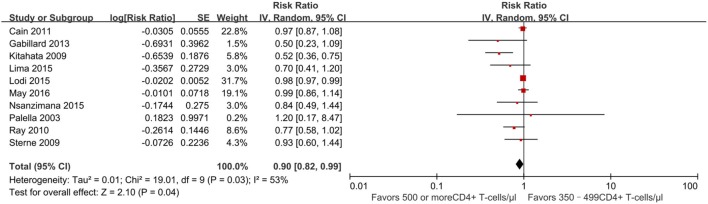
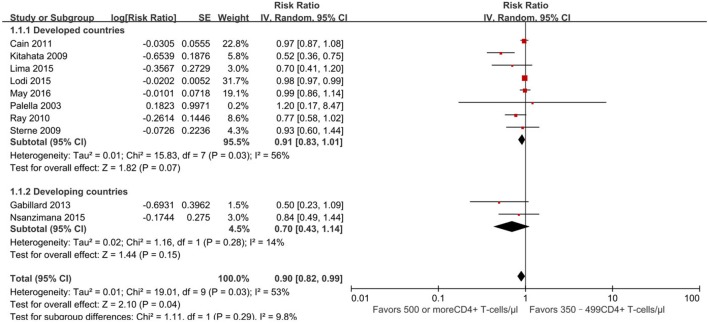
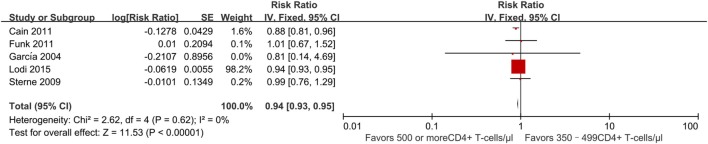
Results: We identified 13 studies comparing early and deferred treatment. The pooled risk ratio (RR) of mortality of 11 observational studies was 0.90 (95% CI 0.82-0.99), with moderate heterogeneity (I2 = 53%). The pooled RR for progression to AIDS from two observational studies was 0.77 (95% CI 0.47-1.24). Five observational studies found a pooled RR of death or AIDS of 0.94 (95% CI 0.93-0.95). For the outcome of immunologic recovery, defined as CD4+ T-cell counts reaching at least 800 cells/mm3 after ART, one observational study found early initiation of ART had an HR (hazard ratio) of 2.39 (95% CI 1.93-2.96). The pooled RR of viral suppression (a viral load <50 copies/ml) after 9 months from one cohort was 1.04 (95% CI 0.99-1.09).
Conclusion: Mortality risk and risk for AIDS appear to be reduced among people living with HIV with early initiation of ART, based on current WHO guidelines, as compared to those with deferred initiation of ART (<500 cells/mm3).
Keywords: CD4+ T cell; HIV-infected adults; early therapy; meta; mortality.
Figures



Similar articles
-
Factors Associated with Timing of Initiation of Antiretroviral Therapy among HIV-1 Infected Adults in the Niger Delta Region of Nigeria.PLoS One. 2015 May 1;10(5):e0125665. doi: 10.1371/journal.pone.0125665. eCollection 2015. PLoS One. 2015. PMID: 25933356 Free PMC article.
-
Clinical outcomes of patients infected with HIV through use of injected drugs compared to patients infected through sexual transmission: late presentation, delayed anti-retroviral treatment and higher mortality.Addiction. 2016 Jul;111(7):1235-45. doi: 10.1111/add.13348. Epub 2016 Apr 14. Addiction. 2016. PMID: 26890155
-
A Trial of Early Antiretrovirals and Isoniazid Preventive Therapy in Africa.N Engl J Med. 2015 Aug 27;373(9):808-22. doi: 10.1056/NEJMoa1507198. Epub 2015 Jul 20. N Engl J Med. 2015. PMID: 26193126 Clinical Trial.
-
Antiretroviral treatment regardless of CD4 count: the universal answer to a contextual question.AIDS Res Ther. 2016 Jul 26;13:27. doi: 10.1186/s12981-016-0111-1. eCollection 2016. AIDS Res Ther. 2016. PMID: 27462361 Free PMC article. Review.
-
CD4+ T cell counts in initiation of antiretroviral therapy in HIV infected asymptomatic individuals; controversies and inconsistencies.Immunol Lett. 2015 Dec;168(2):279-84. doi: 10.1016/j.imlet.2015.10.005. Epub 2015 Oct 22. Immunol Lett. 2015. PMID: 26475399 Review.
Cited by
-
Thymic Exhaustion and Increased Immune Activation Are the Main Mechanisms Involved in Impaired Immunological Recovery of HIV-Positive Patients under ART.Viruses. 2023 Feb 5;15(2):440. doi: 10.3390/v15020440. Viruses. 2023. PMID: 36851655 Free PMC article.
-
The Benefits of Immediate ART.J Int Assoc Provid AIDS Care. 2019 Jan-Dec;18:2325958219831714. doi: 10.1177/2325958219831714. J Int Assoc Provid AIDS Care. 2019. PMID: 30832530 Free PMC article.
-
Microfluidic Assays for CD4 T Lymphocyte Counting: A Review.Biosensors (Basel). 2025 Jan 9;15(1):33. doi: 10.3390/bios15010033. Biosensors (Basel). 2025. PMID: 39852084 Free PMC article. Review.
-
Adjunct Therapy for CD4+ T-Cell Recovery, Inflammation and Immune Activation in People Living With HIV: A Systematic Review and Meta-Analysis.Front Immunol. 2021 Feb 17;12:632119. doi: 10.3389/fimmu.2021.632119. eCollection 2021. Front Immunol. 2021. PMID: 33679779 Free PMC article.
-
How to properly define immunological nonresponse to antiretroviral therapy in people living with HIV? an integrative review.Front Immunol. 2025 Apr 7;16:1535565. doi: 10.3389/fimmu.2025.1535565. eCollection 2025. Front Immunol. 2025. PMID: 40260259 Free PMC article. Review.
References
-
- Hammer SM, Squires KE, Hughes MD, Grimes JM, Demeter LM, Currier JS, et al. A controlled trial of two nucleoside analogues plus indinavir in persons with human immunodeficiency virus infection and CD4 cell counts of 200 per cubic millimeter or less. AIDS clinical trials group 320 study team. N Engl J Med (1997) 337(11):725–33.10.1056/NEJM199709113371101 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials