

Complete response in a patient with liver metastases from breast cancer employing hepatic arterial infusion 5-fluorouracil based chemotherapy plus systemic nab-paclitaxel
- PMID: 29487726
- PMCID: PMC5814293
- DOI: 10.18632/oncotarget.23793
Complete response in a patient with liver metastases from breast cancer employing hepatic arterial infusion 5-fluorouracil based chemotherapy plus systemic nab-paclitaxel
Abstract
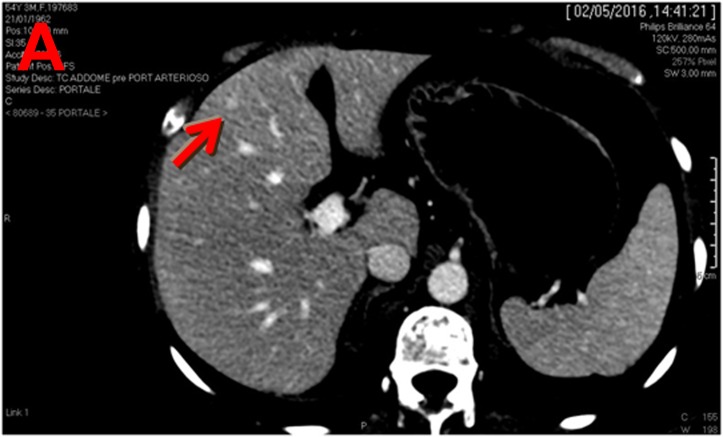
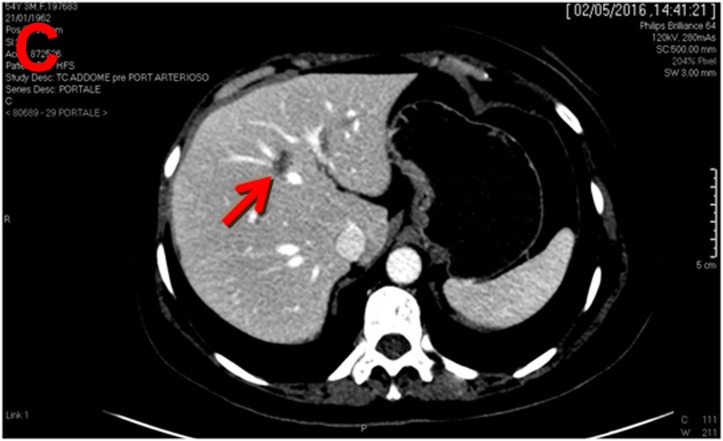
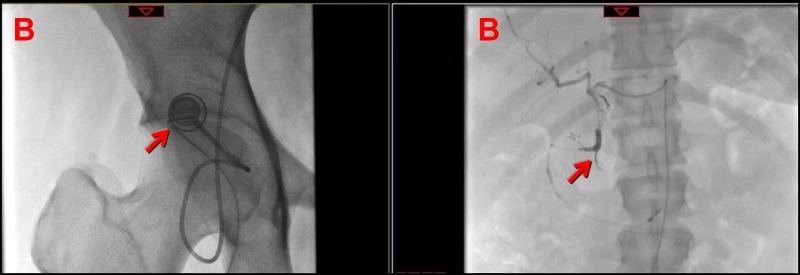
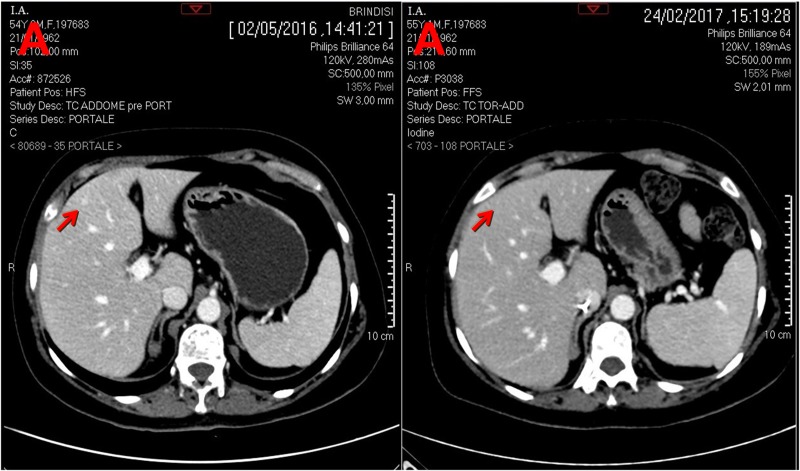
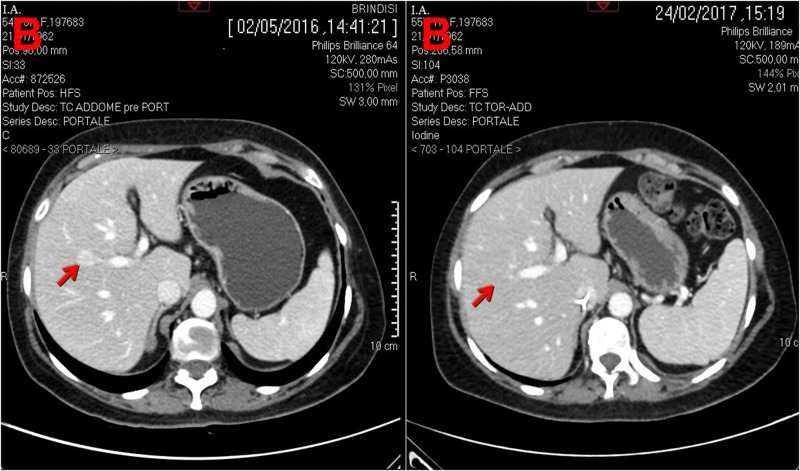
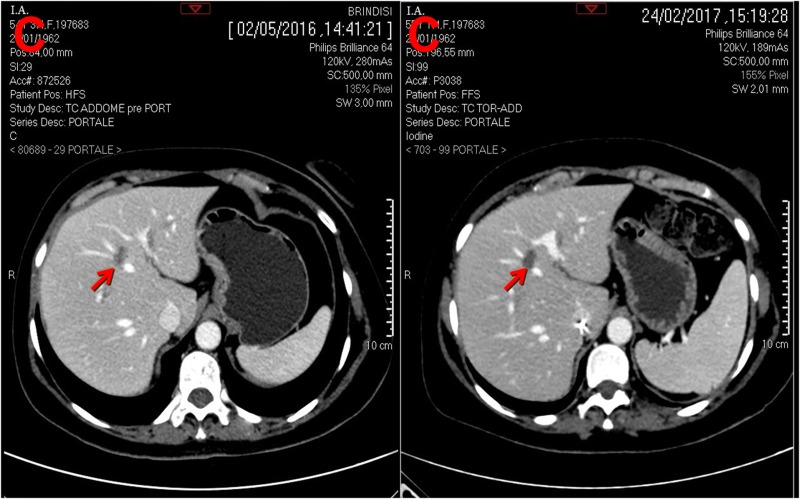
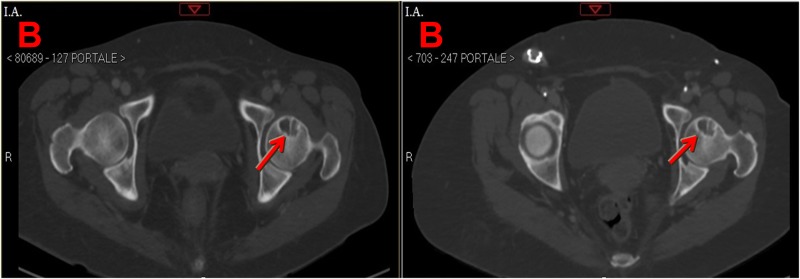
About half of patients with metastatic breast cancer (mBC) have unresectable liver metastases (LMs) or liver-predominant disease (LPD). Unfortunately systemic chemotherapy has limited tumor response due to LMs are supplied by hepatic artery. Hepatic intra-arterial (HAI) have antitumor activity in pretreated patients with LMs. Here we report the case of a 55-year-old woman affected by BCLPD and heavily pretreated. LMs responded to treatment based on HAI with 5-fluorouracil and nab-paclitaxel systemic chemotherapy, and they completely disappeared on a CT-scan. We conclude that this combination chemotherapy is safe and may be very useful for the treatment of patients with BCLPD. Therefore, this combination should be evaluated in a large study.
Keywords: breast cancer; hepatic intra-arterial chemotherapy; liver metastases; nab-paclitaxel.
Conflict of interest statement
CONFLICTS OF INTEREST The authors confirm that there are no conflicts of interest.
Figures



References
-
- Kemeny NE, Melendez FD, Capanu M, Paty PB, Fong Y, Schwartz LH, Jarnagin WR, Patel D, D'Angelica M. Conversion to resectability using hepatic artery infusion plus systemic chemotherapy for the treatment of unresectable liver metastases from colorectal carcinoma. J Clin Oncol. 2009;27:3465–71. doi: 10.1200/JCO.2008.20.1301. - DOI - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
