

A multicenter, randomized trial comparing efficacy and safety of paclitaxel/capecitabine and cisplatin/capecitabine in advanced gastric cancer
- PMID: 29488121
- PMCID: PMC6097104
- DOI: 10.1007/s10120-018-0809-y
A multicenter, randomized trial comparing efficacy and safety of paclitaxel/capecitabine and cisplatin/capecitabine in advanced gastric cancer
Abstract
Background: We compared efficacy and safety of paclitaxel/capecitabine therapy followed by capecitabine for maintenance (PACX) versus cisplatin/capecitabine therapy (XP) in advanced gastric cancer.
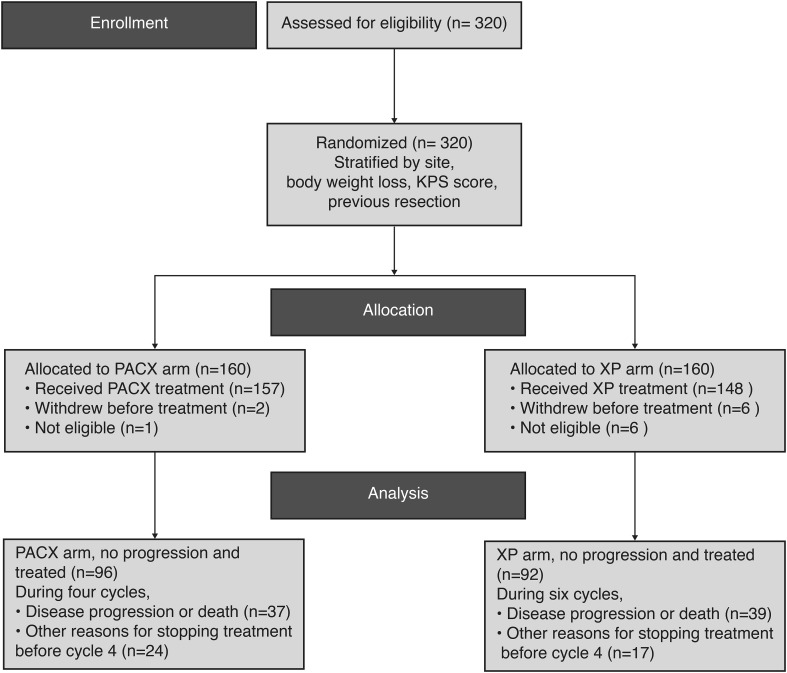
Methods: Multicenter, randomized, phase III trial was conducted in China (December 2009-February 2014). Adults (n = 320) with histologically confirmed, untreated metastatic/unresectable gastric or gastroesophageal junction adenocarcinoma; with ≥ 1 measureable lesions according to Response Evaluation Criteria in Solid Tumors 1.0 criteria; Karnofsky performance score ≥ 70 and life expectancy ≥ 3 months were randomized (1:1) to PACX or XP. PACX group received paclitaxel 80 mg/m2 intravenous on days 1 and 8; capecitabine 1000 mg/m2 orally BD on days 1-14, followed by a 7-day rest interval for 4 cycles, followed by maintenance capecitabine at same dosage/schedule until disease progression, unendurable adverse events or death. XP group received cisplatin intravenous 80 mg/m2 on day 1 and capecitabine at same dosage/schedule as PACX group per cycle for 6 cycles.
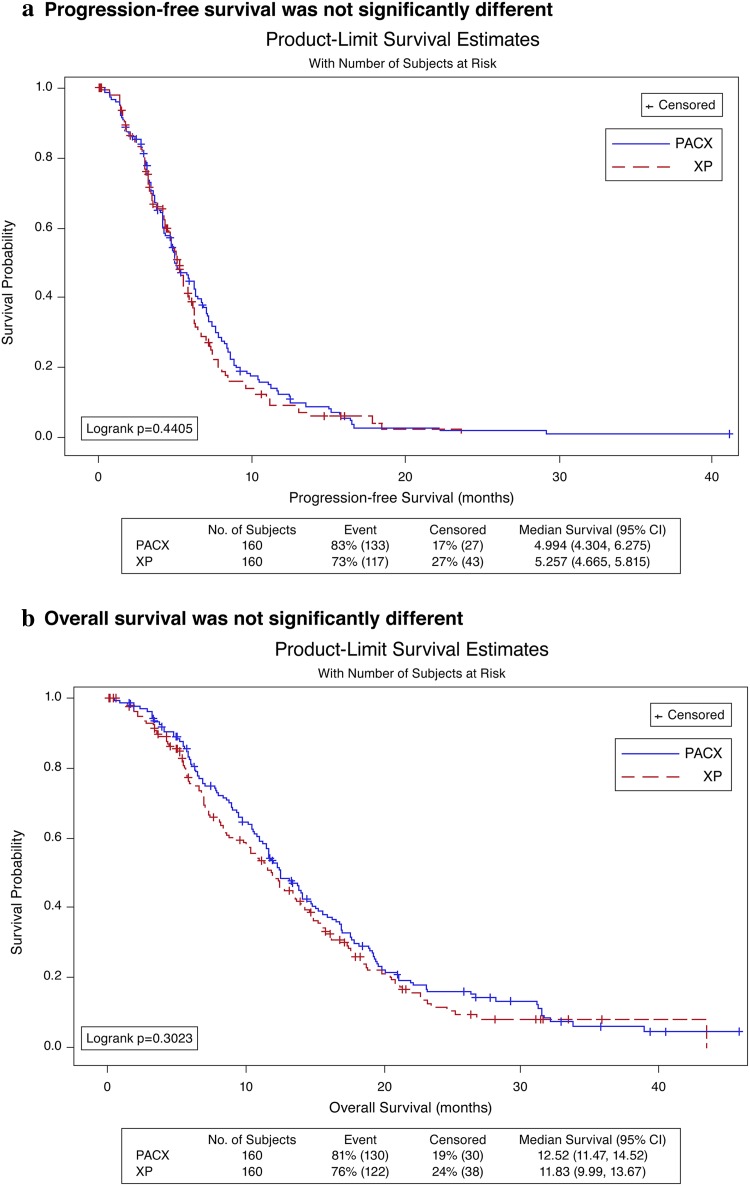
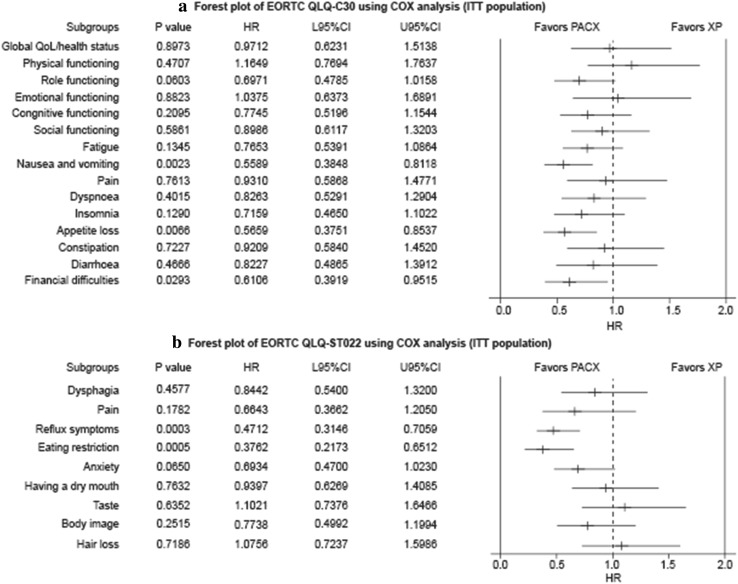
Results: Median progression-free survival (5.0 versus 5.3 months; hazard ratio [95% CI]: 0.906; 0.706-1.164; p = 0.44) and overall survival (12.5 versus 11.8 months; hazard ratio: 0.878 [0.685-1.125]; p = 0.30) were not significantly different between PACX and XP groups. Objective response rate was significantly higher (43.1 versus 28.8%; p = 0.012) and disease control rate was similar (77.5 versus 72.5%; p = 0.75) in PACX versus XP, respectively. Quality of life was significantly improved in PACX versus XP after three treatment cycles. Many treatment-related adverse events were significantly lesser in PACX than XP.
Conclusions: First-line chemotherapy with PACX is effective with milder toxicities in advanced gastric cancer, but could not replace XP.
Keywords: Capecitabine; Cisplatin; Paclitaxel; Stomach neoplasms.
Conflict of interest statement
Conflict of interest
The authors have declared no conflicts of interest. This work was supported by Shanghai Roche Pharmaceuticals Ltd., China and Haiyao Ltd. This study is an investigator initiated study. Roche Ltd. provided the drug capecitabine and part of funding. Haiyao Ltd. provided part of paclitaxel. These two corporations played no role in study design, data collection, data analysis, data interpretation.
Ethical standards
The study protocol was approved by the institutional review board of Peking University Cancer Hospital and respective independent ethics committees at each investigating site. All procedures followed were in accordance with the ethical standards of the responsible committee on human experimentation (institutional and national) and with the Helsinki Declaration of 1964 and later versions.
Informed consent
All participants included in the study provided written informed consent.
Figures
References
-
- Bang YJ, Van Cutsem E, Feyereislova A, Chung HC, Shen L, Sawaki A, et al. Trastuzumab in combination with chemotherapy versus chemotherapy alone for treatment of HER2-positive advanced gastric or gastro-oesophageal junction cancer (ToGA): a phase 3, open-label, randomised controlled trial. Lancet. 2010;376:687–697. doi: 10.1016/S0140-6736(10)61121-X. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
