

Time-dependent changes in bone healing capacity of scaphoid fractures and non-unions
- PMID: 29488208
- PMCID: PMC5979627
- DOI: 10.1111/joa.12795
Time-dependent changes in bone healing capacity of scaphoid fractures and non-unions
Abstract
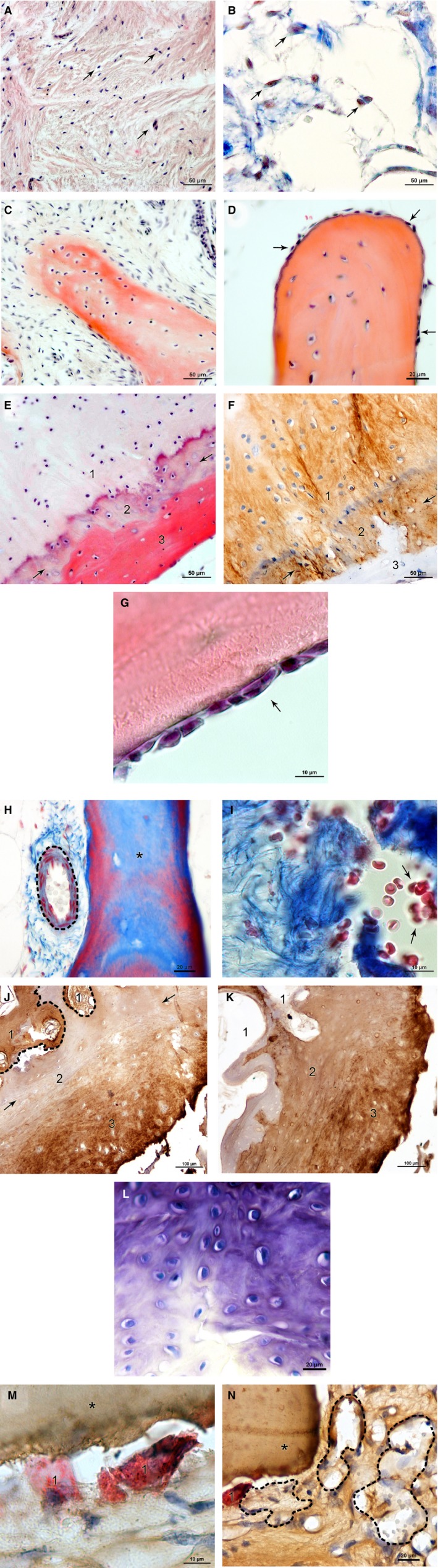
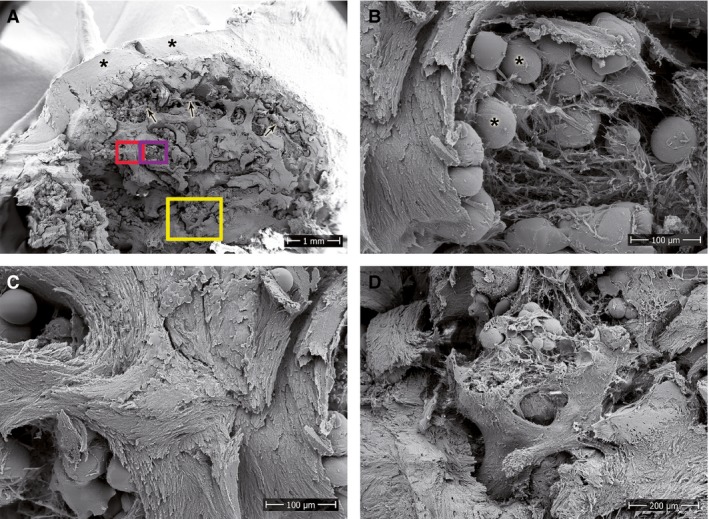
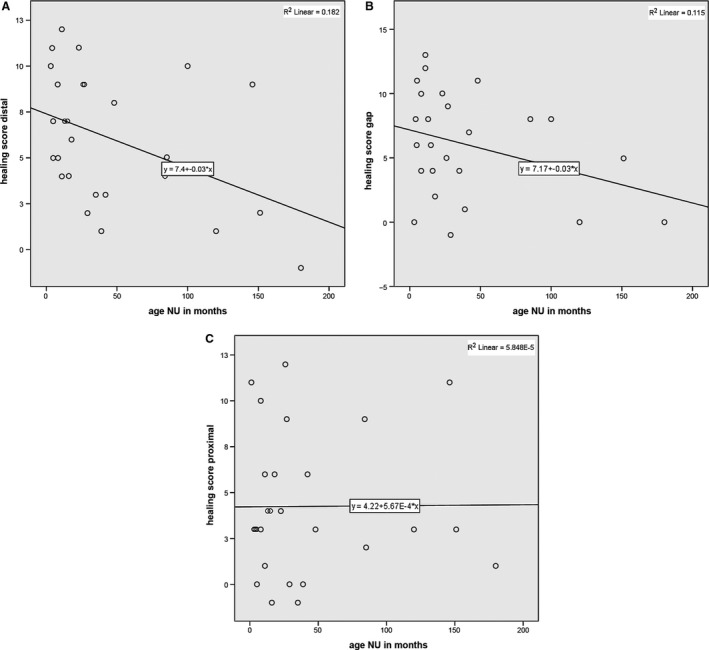
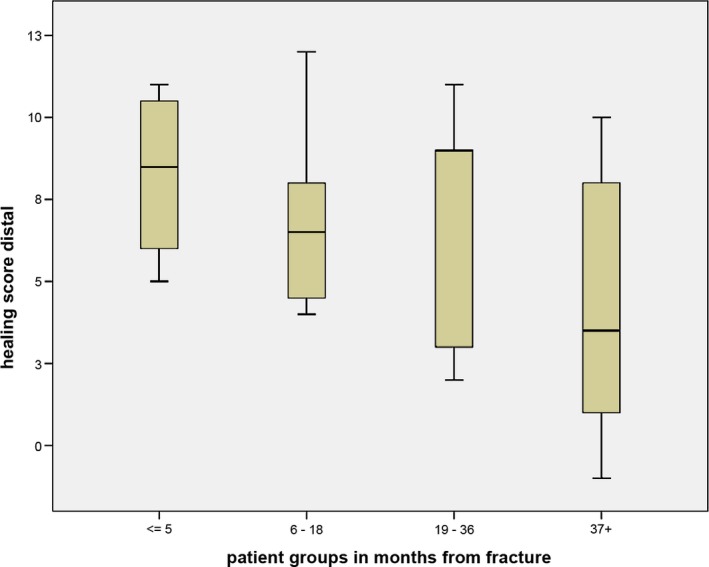
The scaphoid is the most frequently fractured carpal bone and prone to non-union due to mechanical and biological factors. Whereas the importance of stability is well documented, the evaluation of biological activity is mostly limited to the assessment of vascularity. The purpose of this study was to select histological and immunocytochemical parameters that could be used to assess healing potential after scaphoid fractures and to correlate these findings with time intervals after fracture for the three parts of the scaphoid (distal, gap and proximal). Samples were taken during operative intervention in 33 patients with delayed or non-union of the scaphoid. Haematoxylin and Eosin (HE), Azan, Toluidine, von Kossa and Tartrate-resistant acid phosphatase (TRAP) staining were used to characterise the samples histologically. We determined distribution of collagen 1 and 2 by immunocytochemistry, and scanning electron microscopy (SEM) was used to investigate the ultrastructure. To analyse the samples, parameters for biological healing status were defined and grouped according to healing capacity in parameters with high, partial and little biological activity. These findings allowed scoring of biological healing capacity, and the ensuing results were correlated with different time intervals after fracture. The results showed reduced healing capacity over time, but not all parts of the scaphoid were affected in the same way. For the distal fragment, regression analysis showed a statistically significant correlation between summarised healing activity scores and time from initial fracture (r = -0.427, P = 0.026) and decreasing healing activity for the gap region (r = -0.339, P = 0.090). In contrast, the analyses of the proximal parts for all patients did not show a correlation (r = 0.008, P = 0.969) or a decrease in healing capacity, with reduced healing capacity already at early stages. The histological and immunocytochemical characterisation of scaphoid non-unions (SNUs) and the scoring of healing parameters make it possible to analyse the healing capacity of SNUs at certain time points. This information is important as it can assist the surgeon in the selection of the most appropriate SNU treatment.
Keywords: bone healing capacity; histological characterisation; scaphoid fracture; scaphoid non-union; time dependent changes.
© 2018 The Authors. Journal of Anatomy published by John Wiley & Sons Ltd on behalf of Anatomical Society.
Figures
References
-
- Bervian MR, Ribak S, Livani B (2015) Scaphoid fracture nonunion: correlation of radiographic imaging, proximal fragment histologic viability evaluation, and estimation of viability at surgery: diagnosis of scaphoid pseudarthrosis. Int Orthop 39, 67–72. - PubMed
-
- Beutel FK, Wilhelm K (1999) Relation of necrosis to outcome and site of fracture in scaphoid pseudarthrosis. Handchir Mikrochir Plast Chir 31, 207–211. - PubMed
-
- Boyer MI, von Schroeder HP, Axelrod TS (1998) Scaphoid nonunion with avascular necrosis of the proximal pole. Treatment with a vascularized bone graft from the dorsum of the distal radius. J Hand Surg 23, 686–690. - PubMed
-
- Fernandez DL (1990) Anterior bone grafting and conventional lag screw fixation to treat scaphoid nonunions. J Hand Surg Am 15, 140–147. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
