

MySurgeryRisk: Development and Validation of a Machine-learning Risk Algorithm for Major Complications and Death After Surgery
- PMID: 29489489
- PMCID: PMC6110979
- DOI: 10.1097/SLA.0000000000002706
MySurgeryRisk: Development and Validation of a Machine-learning Risk Algorithm for Major Complications and Death After Surgery
Abstract
Objective: To accurately calculate the risk for postoperative complications and death after surgery in the preoperative period using machine-learning modeling of clinical data.
Background: Postoperative complications cause a 2-fold increase in the 30-day mortality and cost, and are associated with long-term consequences. The ability to precisely forecast the risk for major complications before surgery is limited.
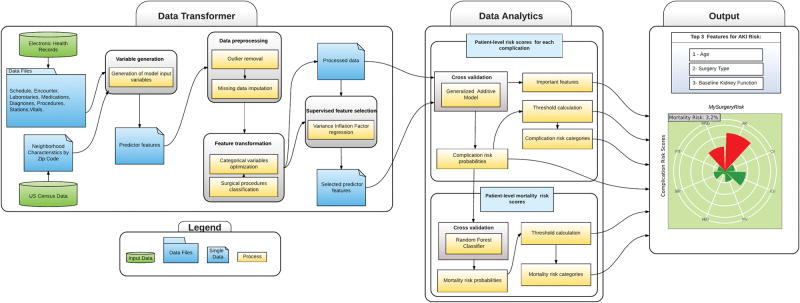
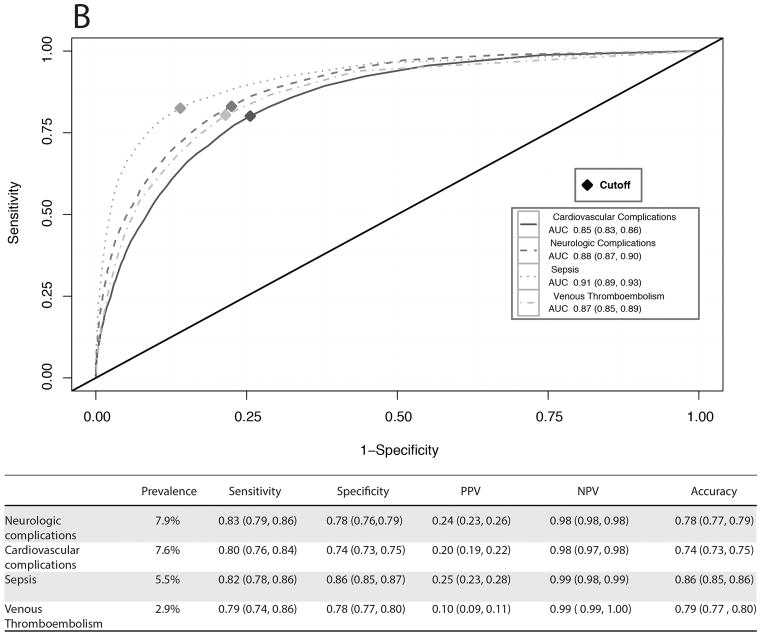
Methods: In a single-center cohort of 51,457 surgical patients undergoing major inpatient surgery, we have developed and validated an automated analytics framework for a preoperative risk algorithm (MySurgeryRisk) that uses existing clinical data in electronic health records to forecast patient-level probabilistic risk scores for 8 major postoperative complications (acute kidney injury, sepsis, venous thromboembolism, intensive care unit admission >48 hours, mechanical ventilation >48 hours, wound, neurologic, and cardiovascular complications) and death up to 24 months after surgery. We used the area under the receiver characteristic curve (AUC) and predictiveness curves to evaluate model performance.
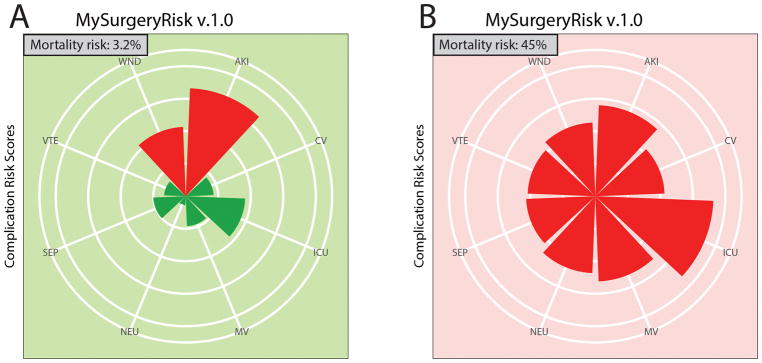
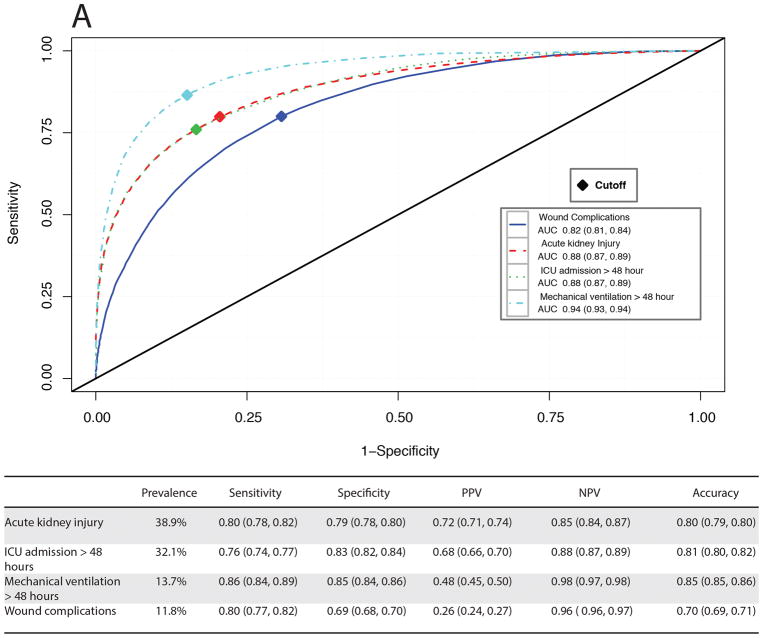
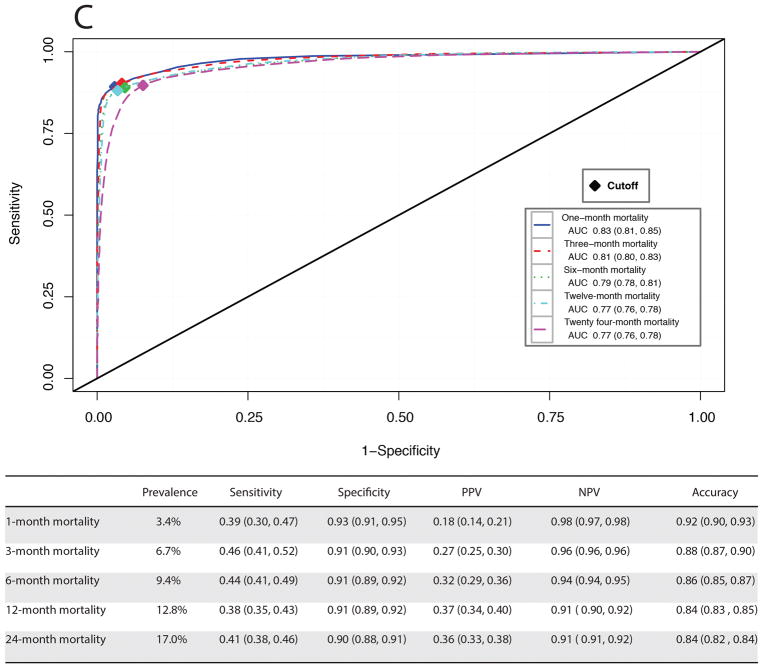
Results: MySurgeryRisk calculates probabilistic risk scores for 8 postoperative complications with AUC values ranging between 0.82 and 0.94 [99% confidence intervals (CIs) 0.81-0.94]. The model predicts the risk for death at 1, 3, 6, 12, and 24 months with AUC values ranging between 0.77 and 0.83 (99% CI 0.76-0.85).
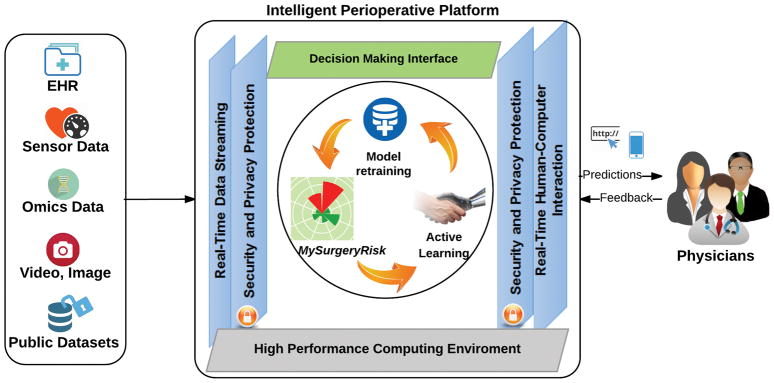
Conclusions: We constructed an automated predictive analytics framework for machine-learning algorithm with high discriminatory ability for assessing the risk of surgical complications and death using readily available preoperative electronic health records data. The feasibility of this novel algorithm implemented in real time clinical workflow requires further testing.
Conflict of interest statement
Conflict of Interest Disclosures: None reported.
Figures
Comment in
-
MySurgeryRisk and Machine Learning: A Promising Start to Real-time Clinical Decision Support.Ann Surg. 2019 Jan;269(1):e14-e15. doi: 10.1097/SLA.0000000000002877. Ann Surg. 2019. PMID: 30048316 No abstract available.
-
Comment on "Is Medicine Still an Art?".Ann Surg. 2019 Jun;269(6):e74. doi: 10.1097/SLA.0000000000002879. Ann Surg. 2019. PMID: 31082923 No abstract available.
-
Response to Comment on "MySurgeryRisk: Development and Validation of a Machine-learning Risk Algorithm for Major Complications and Death After Surgery".Ann Surg. 2019 Jun;269(6):e74. doi: 10.1097/SLA.0000000000002884. Ann Surg. 2019. PMID: 31082924 Free PMC article. No abstract available.
References
-
- Lee PH, Gawande AA. The number of surgical procedures in an American lifetime in 3 states. Journal of the American College of Surgeons. 2008;207(3):S75–S75.
-
- Weiser TG, Regenbogen SE, Thompson KD, et al. An estimation of the global volume of surgery: a modelling strategy based on available data. The Lancet. 2008;372(9633):139–144. - PubMed
-
- Grocott MPW, Pearse RM. Perioperative medicine: the future of anaesthesia? British Journal of Anaesthesia. 2012;108(5):723–726. - PubMed
-
- Lake AP, Williams EG. ASA classification and perioperative variables: graded anaesthesia score? Br J Anaesth. 1997;78(2):228–9. - PubMed
-
- Moonesinghe SR, Mythen MG, Das P, et al. Risk stratification tools for predicting morbidity and mortality in adult patients undergoing major surgery: qualitative systematic review. Anesthesiology. 2013;119(4):959–81. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
