

Diet during pregnancy and infancy and risk of allergic or autoimmune disease: A systematic review and meta-analysis
- PMID: 29489823
- PMCID: PMC5830033
- DOI: 10.1371/journal.pmed.1002507
Diet during pregnancy and infancy and risk of allergic or autoimmune disease: A systematic review and meta-analysis
Abstract
Background: There is uncertainty about the influence of diet during pregnancy and infancy on a child's immune development. We assessed whether variations in maternal or infant diet can influence risk of allergic or autoimmune disease.
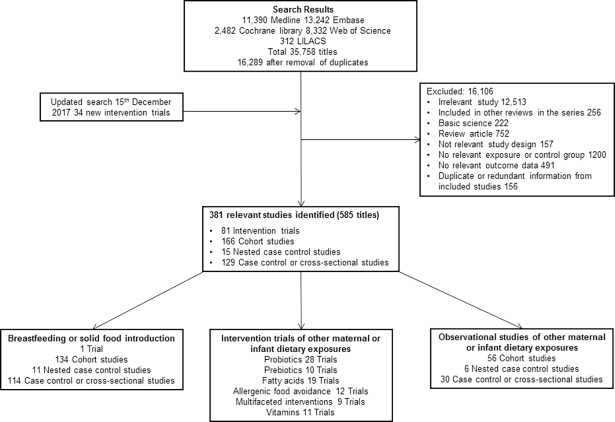
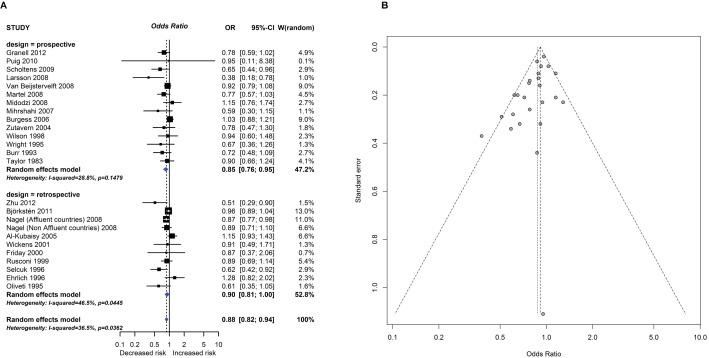
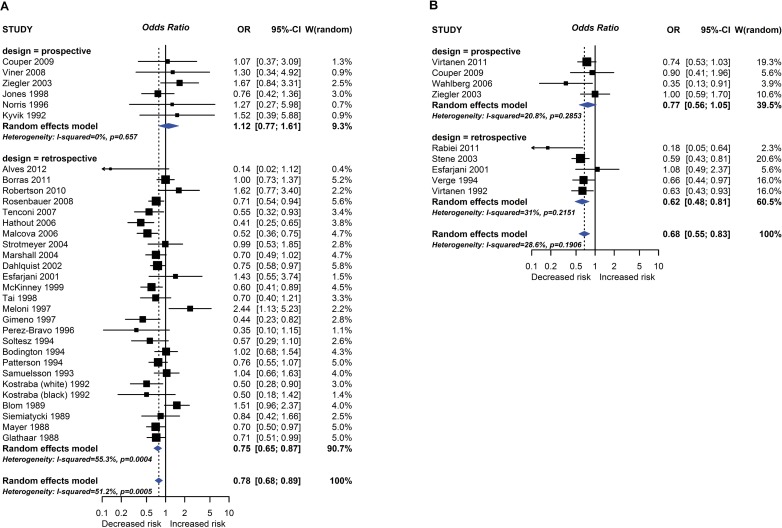
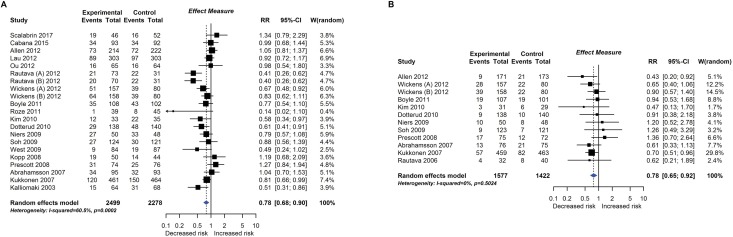
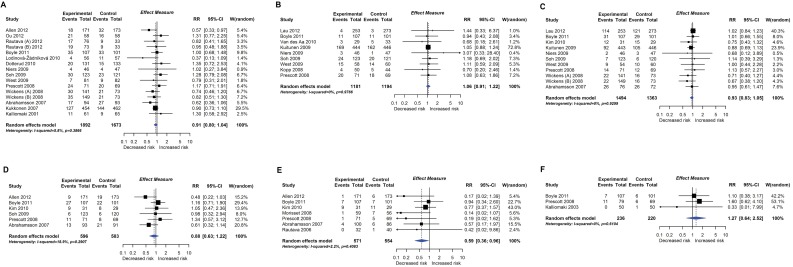
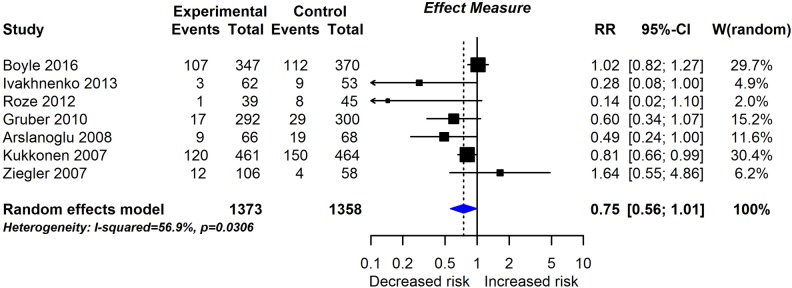
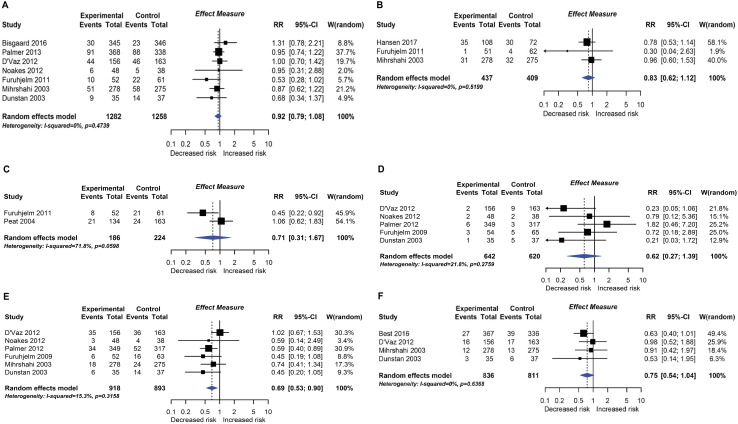
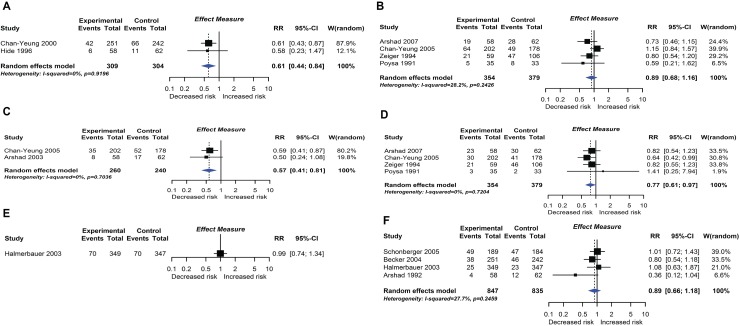
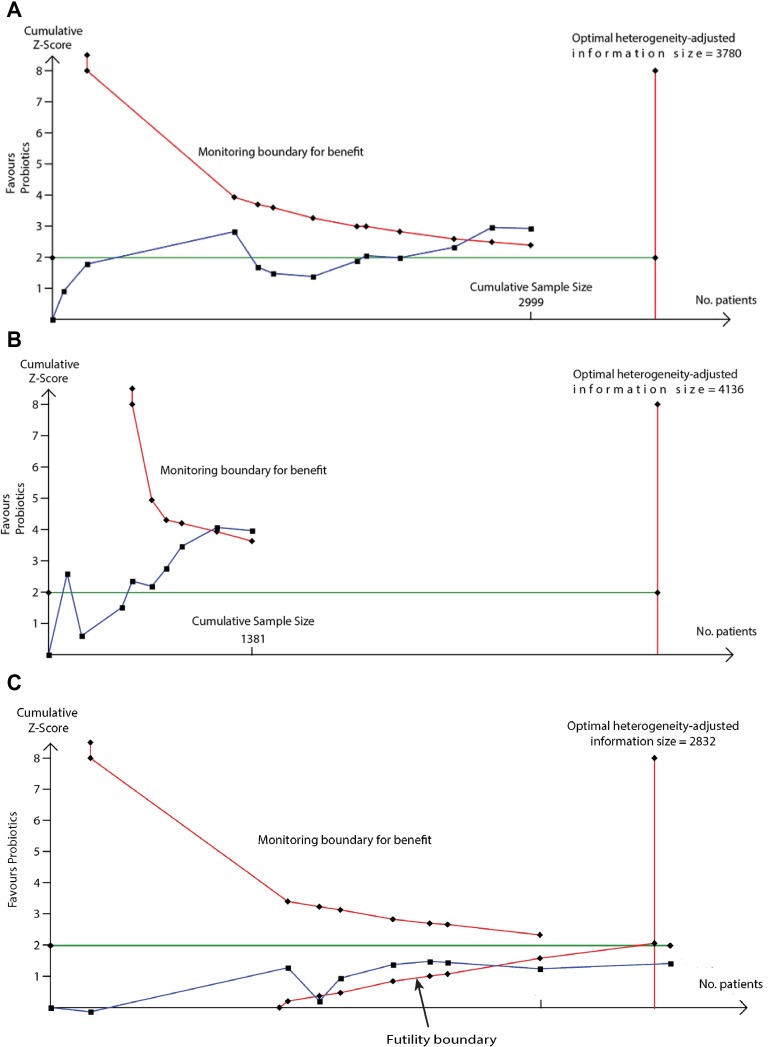
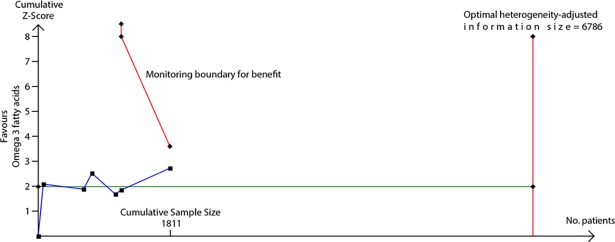
Methods and findings: Two authors selected studies, extracted data, and assessed risk of bias. Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess certainty of findings. We searched Medical Literature Analysis and Retrieval System Online (MEDLINE), Excerpta Medica dataBASE (EMBASE), Web of Science, Central Register of Controlled Trials (CENTRAL), and Literatura Latino Americana em Ciências da Saúde (LILACS) between January 1946 and July 2013 for observational studies and until December 2017 for intervention studies that evaluated the relationship between diet during pregnancy, lactation, or the first year of life and future risk of allergic or autoimmune disease. We identified 260 original studies (964,143 participants) of milk feeding, including 1 intervention trial of breastfeeding promotion, and 173 original studies (542,672 participants) of other maternal or infant dietary exposures, including 80 trials of maternal (n = 26), infant (n = 32), or combined (n = 22) interventions. Risk of bias was high in 125 (48%) milk feeding studies and 44 (25%) studies of other dietary exposures. Evidence from 19 intervention trials suggests that oral supplementation with nonpathogenic micro-organisms (probiotics) during late pregnancy and lactation may reduce risk of eczema (Risk Ratio [RR] 0.78; 95% CI 0.68-0.90; I2 = 61%; Absolute Risk Reduction 44 cases per 1,000; 95% CI 20-64), and 6 trials suggest that fish oil supplementation during pregnancy and lactation may reduce risk of allergic sensitisation to egg (RR 0.69, 95% CI 0.53-0.90; I2 = 15%; Absolute Risk Reduction 31 cases per 1,000; 95% CI 10-47). GRADE certainty of these findings was moderate. We found weaker support for the hypotheses that breastfeeding promotion reduces risk of eczema during infancy (1 intervention trial), that longer exclusive breastfeeding is associated with reduced type 1 diabetes mellitus (28 observational studies), and that probiotics reduce risk of allergic sensitisation to cow's milk (9 intervention trials), where GRADE certainty of findings was low. We did not find that other dietary exposures-including prebiotic supplements, maternal allergenic food avoidance, and vitamin, mineral, fruit, and vegetable intake-influence risk of allergic or autoimmune disease. For many dietary exposures, data were inconclusive or inconsistent, such that we were unable to exclude the possibility of important beneficial or harmful effects. In this comprehensive systematic review, we were not able to include more recent observational studies or verify data via direct contact with authors, and we did not evaluate measures of food diversity during infancy.
Conclusions: Our findings support a relationship between maternal diet and risk of immune-mediated diseases in the child. Maternal probiotic and fish oil supplementation may reduce risk of eczema and allergic sensitisation to food, respectively.
Conflict of interest statement
I have read the journal's policy and the authors of this manuscript have the following competing interests: RJB, VGL, JLB, SC, and DI received support from the UK Food Standards Agency for the submitted work. MT received a consultation fee from the UK Food Standards Agency for methodological work on this systematic review. No other support was received from any organisation for the submitted work. The authors have no financial relationships with any organisations that might have an interest in the submitted work in the previous three years. RJB was a co-investigator and author of two of the trials included in this systematic review. The authors report no other relationships or activities that could appear to have influenced the submitted work.
Figures

References
-
- Prescott SL. Early-life environmental determinants of allergic diseases and the wider pandemic of inflammatory noncommunicable diseases. J Allergy Clin Immunol. 2013; 131(1): 23–30. doi: 10.1016/j.jaci.2012.11.019 - DOI - PubMed
-
- Cuello-Garcia CA, Fiocchi A, Pawankar R, Yepes-Nunez JJ, Morgano GP, et al. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): Prebiotics. World Allergy Organ J. 2016; 9: 10 doi: 10.1186/s40413-016-0102-7 - DOI - PMC - PubMed
-
- Fiocchi A, Pawankar R, Cuello-Garcia C, Ahn K, Al-Hammadi S, et al. World Allergy Organization-McMaster University Guidelines for Allergic Disease Prevention (GLAD-P): Probiotics. World Allergy Organ J. 2015; 8(1): 4 doi: 10.1186/s40413-015-0055-2 - DOI - PMC - PubMed
-
- Muraro A, Halken S, Arshad SH, Beyer K, Dubois AE, et al. EAACI food allergy and anaphylaxis guidelines. Primary prevention of food allergy. Allergy. 2014; 69(5): 590–601. doi: 10.1111/all.12398 - DOI - PubMed
-
- Greer FR, Sicherer SH, Burks AW, Comm N. Effects of early nutritional interventions on the development of atopic disease in infants and children: The role of maternal dietary restriction, breastfeeding, timing of introduction of complementary foods, and hydrolyzed formulas. Pediatrics. 2008; 121(1): 183–191. doi: 10.1542/peds.2007-3022 - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
