

Effects of clinical pathway implementation on antibiotic prescriptions for pediatric community-acquired pneumonia
- PMID: 29489898
- PMCID: PMC5831636
- DOI: 10.1371/journal.pone.0193581
Effects of clinical pathway implementation on antibiotic prescriptions for pediatric community-acquired pneumonia
Abstract
Background: Italian pediatric antimicrobial prescription rates are among the highest in Europe. As a first step in an Antimicrobial Stewardship Program, we implemented a Clinical Pathway (CP) for Community Acquired Pneumonia with the aim of decreasing overall prescription of antibiotics, especially broad-spectrum.
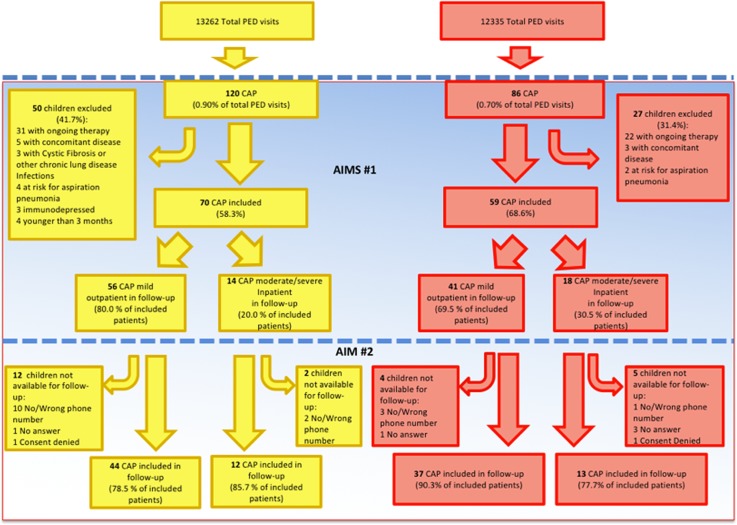
Materials and methods: The CP was implemented on 10/01/2015. We collected antibiotic prescribing and outcomes data from children aged 3 months-15 years diagnosed with CAP from 10/15/2014 to 04/15/2015 (pre-intervention period) and from 10/15/2015 to 04/15/2016 (post-intervention period). We assessed antibiotic prescription differences pre- and post-CP, including rates, breadth of spectrum, and duration of therapy. We also compared length of hospital stay for inpatients and treatment failure for inpatients and outpatients. Chi-square and Fisher's exact test were used to compare categorical variables and Wilcoxon rank sum test was used to compare quantitative outcomes.
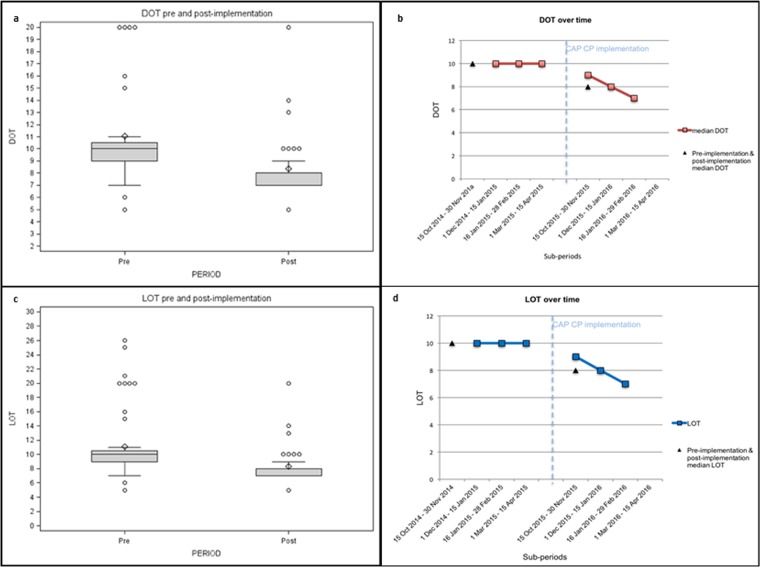
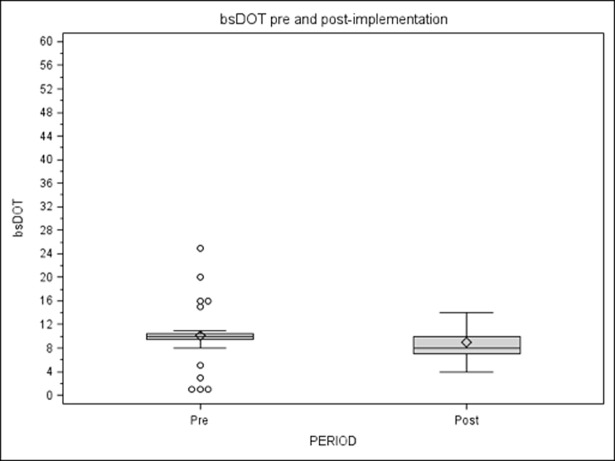
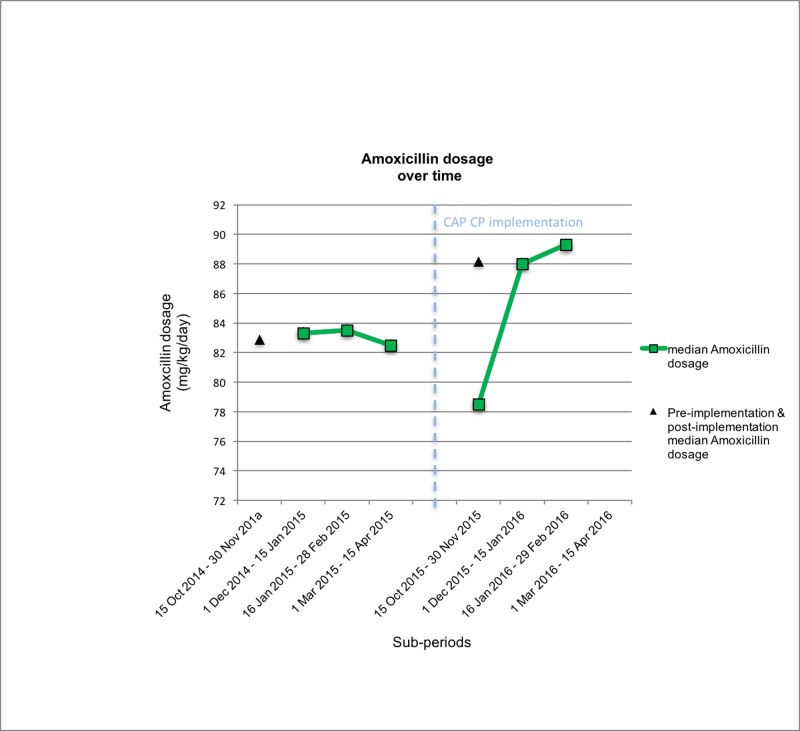
Results: 120 pre- and 86 post-intervention clinic visits were identified with a diagnosis of CAP. In outpatients, we observed a decrease in broad-spectrum regimens (50% pre-CP vs. 26.8% post-CP, p = 0.02), in particular macrolides, and an increase in narrow-spectrum (amoxicillin) post-CP. Post-CP children received fewer antibiotic courses (median DOT from 10 pre-CP to 8 post-CP, p<0.0001) for fewer days (median LOT from 10 pre-CP to 8 post-CP, p<0.0001) than their pre-CP counterparts. Physicians prescribed narrow-spectrum monotherapy more frequently than broad-spectrum combination therapy (DOT/LOT ratio 1.157 pre-CP vs. 1.065 post-CP). No difference in treatment failure was reported before and after implementation (2.3% pre-CP vs. 11.8% post-CP, p = 0.29). Among inpatients we also noted a decrease in broad-spectrum regimens (100% pre-CP vs. 66.7% post-CP, p = 0.02) and the introduction of narrow-spectrum regimens (0% pre-CP vs. 33.3% post-CP, p = 0.02) post-CP. Hospitalized patients received fewer antibiotic courses post-CP (median DOT from 18.5 pre-CP to 10 post-CP, p = 0.004), while there was no statistical difference in length of therapy (median LOT from 11 pre-CP to 10 post-CP, p = 0.06). Days of broad spectrum therapy were notably lower post-CP (median bsDOT from 17 pre-CP to 4.5 post-CP, p <0.0001). No difference in treatment failure was reported before and after CP implementation (16.7% pre-CP vs. 15.4% post-CP, p = 1).
Conclusions: Introduction of a CP for CAP in a Pediatric Emergency Department led to reduction of broad-spectrum antibiotic prescriptions, of combination therapy and of duration of treatment both for outpatients and inpatients.
Conflict of interest statement
Figures
Similar articles
-
Multistep antimicrobial stewardship intervention on antibiotic prescriptions and treatment duration in children with pneumonia.PLoS One. 2021 Oct 27;16(10):e0257993. doi: 10.1371/journal.pone.0257993. eCollection 2021. PLoS One. 2021. PMID: 34705849 Free PMC article.
-
The Impact of Clinical Pathways on Antibiotic Prescribing for Acute Otitis Media and Pharyngitis in the Emergency Department.Pediatr Infect Dis J. 2018 Sep;37(9):901-907. doi: 10.1097/INF.0000000000001976. Pediatr Infect Dis J. 2018. PMID: 29561517
-
Antibiotic Choice and Clinical Outcomes in Ambulatory Children with Community-Acquired Pneumonia.J Pediatr. 2021 Feb;229:207-215.e1. doi: 10.1016/j.jpeds.2020.10.005. Epub 2020 Oct 10. J Pediatr. 2021. PMID: 33045236 Free PMC article.
-
What is the role of antimicrobial stewardship in improving outcomes of patients with CAP?Infect Dis Clin North Am. 2013 Mar;27(1):211-28. doi: 10.1016/j.idc.2012.11.008. Infect Dis Clin North Am. 2013. PMID: 23398876 Review.
-
Treatment of mild to moderate community-acquired pneumonia in previously healthy children: an Italian intersociety consensus (SIPPS-SIP-SITIP-FIMP-SIAIP-SIMRI-FIMMG-SIMG).Ital J Pediatr. 2024 Oct 19;50(1):217. doi: 10.1186/s13052-024-01786-8. Ital J Pediatr. 2024. PMID: 39427174 Free PMC article.
Cited by
-
Event Surrogate from Clinical Pathway Completion to Daily Meal for Availability Extension Using Standard Electronic Medical Records: a Retrospective Cohort Study.J Med Syst. 2021 Feb 5;45(3):33. doi: 10.1007/s10916-021-01714-x. J Med Syst. 2021. PMID: 33547499
-
Exploring patient's clinical outcomes, hospital costs, and satisfaction after the implementation of integrated clinical pathway-based nursing practice model.Cost Eff Resour Alloc. 2025 Jul 30;23(1):38. doi: 10.1186/s12962-025-00645-5. Cost Eff Resour Alloc. 2025. PMID: 40739272 Free PMC article.
-
Effective Clinical Pathway Improves Interprofessional Collaboration and Reduces Antibiotics Prophylaxis Use in Orthopedic Surgery in Hospitals in Indonesia.Antibiotics (Basel). 2022 Mar 16;11(3):399. doi: 10.3390/antibiotics11030399. Antibiotics (Basel). 2022. PMID: 35326862 Free PMC article.
-
Multistep antimicrobial stewardship intervention on antibiotic prescriptions and treatment duration in children with pneumonia.PLoS One. 2021 Oct 27;16(10):e0257993. doi: 10.1371/journal.pone.0257993. eCollection 2021. PLoS One. 2021. PMID: 34705849 Free PMC article.
-
Big-data analysis: A clinical pathway on endoscopic retrograde cholangiopancreatography for common bile duct stones.World J Gastroenterol. 2019 Feb 28;25(8):1002-1011. doi: 10.3748/wjg.v25.i8.1002. World J Gastroenterol. 2019. PMID: 30833805 Free PMC article.
References
-
- Bradley JS, Byington CL, Shah SS, Alverson B, Carter ER, Harrison C, et al. Pediatric Infectious Diseases Society and the Infectious Diseases Society of America: The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society of America. Clin Infect Dis 2011; 53(7): e25–76 doi: 10.1093/cid/cir531 - DOI - PMC - PubMed
-
- Wardlaw T, Salama P, Johansson EW, Mason E. Pneumonia: the leading killer of children. Lancet 2006; 368: 1048–1050 doi: 10.1016/S0140-6736(06)69334-3 - DOI - PubMed
-
- Don M, Canciani M, Korppi M. Community-acquired pneumonia in children: what’s old? What’s new? Acta Paediatrica 2010; 99: 1602–1608 doi: 10.1111/j.1651-2227.2010.01924.x - DOI - PubMed
-
- Leyenaar JK, Lagu T, Shieh MS, Pekow PS, Lindenauer PK: Variation in resource utilization for the management of uncomplicated community-acquired pneumonia across community and children’s hospitals. J Pediatr 2014; 165(3): 585–591 doi: 10.1016/j.jpeds.2014.04.062 - DOI - PMC - PubMed
-
- Stein RT, Marostica PJ. Community-acquired pneumonia: a review and recent advances. Pediatr Pulmonol 2007; 42: 1095–1103 doi: 10.1002/ppul.20652 - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
