

Potential for reducing inappropriate antibiotic prescribing in English primary care
- PMID: 29490058
- PMCID: PMC5890667
- DOI: 10.1093/jac/dkx500
Potential for reducing inappropriate antibiotic prescribing in English primary care
Abstract
Objectives: To identify and quantify inappropriate systemic antibiotic prescribing in primary care in England, and ultimately to determine the potential for reduction in prescribing of antibiotics.
Methods: Primary care data from 2013-15 recorded in The Health Improvement Network (THIN) database were used. Potentially inappropriate prescribing events in the database were identified by: (i) comparing prescribing events against treatment guidelines; (ii) comparing actual proportions of consultations resulting in prescription for a set of conditions with the ideal proportions derived from expert opinion; and (iii) identifying high prescribers and their number of prescriptions above an age- and body-system-specific benchmark.
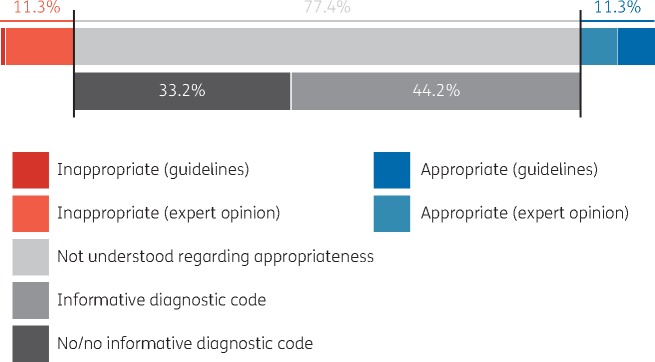
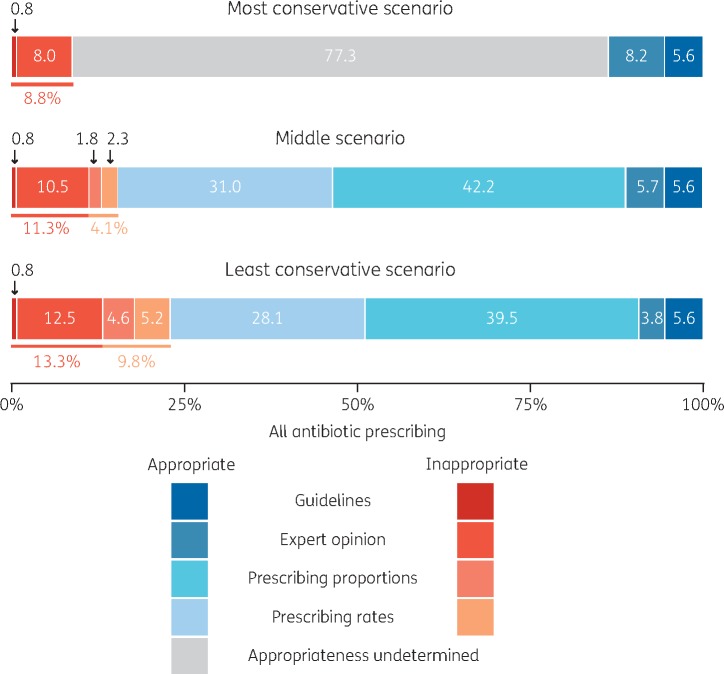
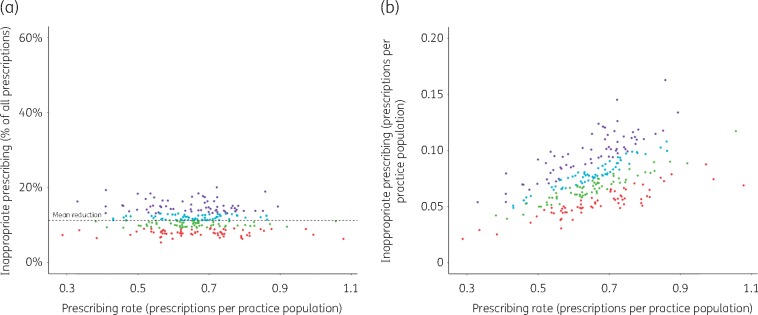
Results: Applying the most conservative assumptions, 8.8% of all systemic antibiotic prescriptions in English primary care were identified as inappropriate, and in the least conservative scenario 23.1% of prescriptions were inappropriate. All practices had non-zero reduction potentials, ranging from 6.4% to 43.5% in the middle scenario. The four conditions that contributed most to inappropriate prescribing were sore throat (23.0% of identified inappropriate prescriptions), cough (22.2%), sinusitis (7.6%) and acute otitis media (5.7%). One-third of all antibiotic prescriptions lacked an informative diagnostic code.
Conclusions: This work demonstrates (i) the existence of substantial inappropriate antibiotic prescribing and (ii) poor diagnostic coding in English primary care. All practices (not just the high prescribers) should engage in efforts to improve antimicrobial stewardship. Better diagnostic coding, more precise prescribing guidelines and a deeper understanding of appropriate long-term uses of antibiotics would allow identification of further potential for reductions.
Figures
References
-
- Costelloe C, Metcalf C, Lovering A. et al. Effects of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ 2010; 340: c2096.. - PubMed
-
- Van Boeckel TP, Gandra S, Ashok A. et al. Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data. Lancet Infect Dis 2014; 14: 742–50. - PubMed
-
- Wang J, Wang P, Wang X. et al. Use and prescription of antibiotics in primary health care settings in China. JAMA Intern Med 2004; 174: 1914–20. - PubMed
-
- Fleming-Dutra KE, Hersh AL, Shapiro DJ. et al. Prevalence of inappropriate antibiotic prescriptions among US ambulatory care visits, 2010-2011. JAMA 2016; 315: 1864–73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
