

Temporal Delays Along the Neurosurgical Care Continuum for Traumatic Brain Injury Patients at a Tertiary Care Hospital in Kampala, Uganda
- PMID: 29490070
- PMCID: PMC6292785
- DOI: 10.1093/neuros/nyy004
Temporal Delays Along the Neurosurgical Care Continuum for Traumatic Brain Injury Patients at a Tertiary Care Hospital in Kampala, Uganda
Abstract
Background: Significant care continuum delays between acute traumatic brain injury (TBI) and definitive surgery are associated with poor outcomes. Use of the "3 delays" model to evaluate TBI outcomes in low- and middle-income countries has not been performed.
Objective: To describe the care continuum, using the 3 delays framework, and its association with TBI patient outcomes in Kampala, Uganda.
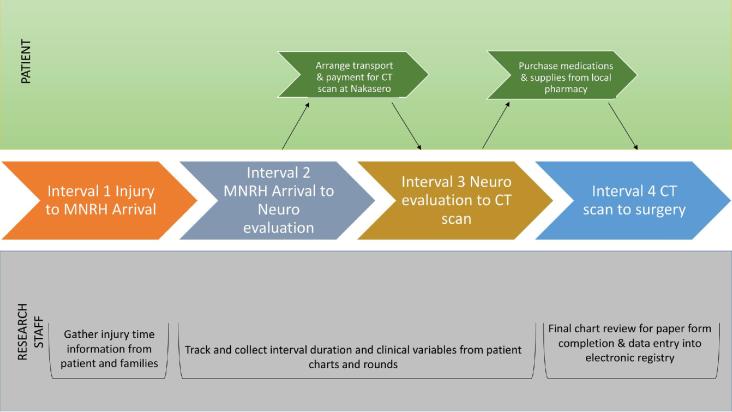
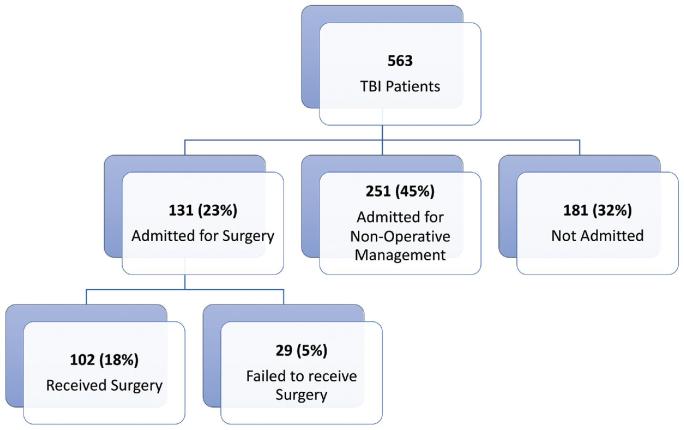
Methods: Prospective data were collected for 563 TBI patients presenting to a tertiary hospital in Kampala from 1 June to 30 November 2016. Four time intervals were constructed along 5 time points: injury, hospital arrival, neurosurgical evaluation, computed tomography (CT) results, and definitive surgery. Time interval differences among mild, moderate, and severe TBI and their association with mortality were analyzed.
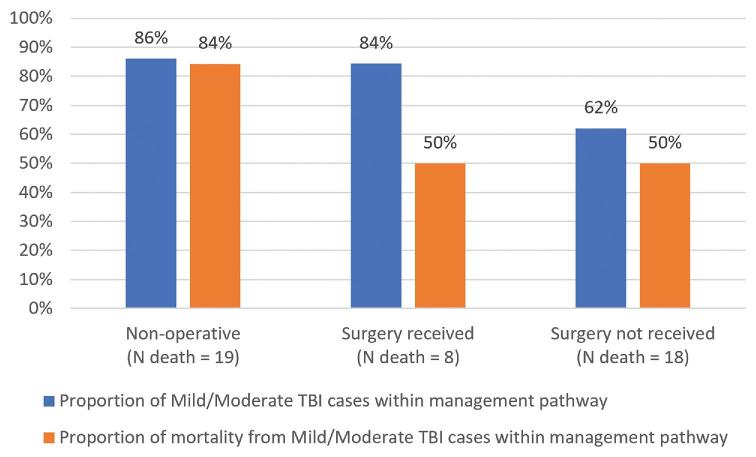
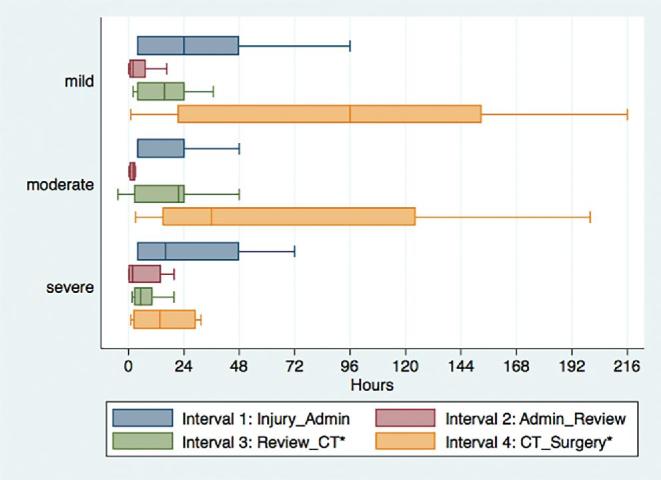
Results: Significant care continuum differences were observed for interval 3 (neurosurgical evaluation to CT result) and 4 (CT result to surgery) between severe TBI patients (7 h for interval 3 and 24 h for interval 4) and mild TBI patients (19 h for interval 3 and 96 h for interval 4). These postarrival delays were associated with mortality for mild (P = .05) and moderate TBI (P = .03) patients. Significant hospital arrival delays for moderate TBI patients were associated with mortality (P = .04).
Conclusion: Delays for mild and moderate TBI patients were associated with mortality, suggesting that quality improvement interventions could target current triage practices. Future research should aim to understand the contributors to delays along the care continuum, opportunities for more effective resource allocation, and the need to improve prehospital logistical referral systems.
Figures
Similar articles
-
A prospective neurosurgical registry evaluating the clinical care of traumatic brain injury patients presenting to Mulago National Referral Hospital in Uganda.PLoS One. 2017 Oct 31;12(10):e0182285. doi: 10.1371/journal.pone.0182285. eCollection 2017. PLoS One. 2017. PMID: 29088217 Free PMC article.
-
Epidemiology and delays in neurosurgical care among patients with traumatic brain injury in a regional referral hospital in Sri Lanka: a retrospective cohort study.Neurosurg Focus. 2025 Mar 1;58(3):E3. doi: 10.3171/2024.12.FOCUS24785. Neurosurg Focus. 2025. PMID: 40022752
-
Long-term follow-up of neurosurgical outcomes for adult patients in Uganda with traumatic brain injury.J Neurosurg. 2020 Jul 3;134(6):1929-1939. doi: 10.3171/2020.4.JNS193092. Print 2021 Jun 1. J Neurosurg. 2020. PMID: 32619973
-
Traumatic brain injury in Indian children.Childs Nerv Syst. 2018 Jun;34(6):1119-1123. doi: 10.1007/s00381-018-3784-z. Epub 2018 Mar 29. Childs Nerv Syst. 2018. PMID: 29594463 Review.
-
Temporal Delays in the Management of Traumatic Brain Injury: A Comparative Meta-Analysis of Global Literature.World Neurosurg. 2024 Aug;188:185-198.e10. doi: 10.1016/j.wneu.2024.05.064. Epub 2024 May 16. World Neurosurg. 2024. PMID: 38762022 Review.
Cited by
-
Neurotrauma from fall accidents in Ethiopia.Brain Spine. 2024 Apr 10;4:102792. doi: 10.1016/j.bas.2024.102792. eCollection 2024. Brain Spine. 2024. PMID: 38983751 Free PMC article.
-
Development of clinical decision rules for traumatic intracranial injuries in patients with mild traumatic brain injury in a developing country.PLoS One. 2020 Sep 18;15(9):e0239082. doi: 10.1371/journal.pone.0239082. eCollection 2020. PLoS One. 2020. PMID: 32946468 Free PMC article.
-
Exploring the feasibility of pupillometry training and perceptions of potential use for intracranial pressure monitoring in Uganda: A mixed methods study.PLoS One. 2024 May 15;19(5):e0298619. doi: 10.1371/journal.pone.0298619. eCollection 2024. PLoS One. 2024. PMID: 38748676 Free PMC article.
-
Affordability impacts therapeutic intensity of acute management of severe traumatic brain injury patients: An exploratory study in Tanzania.Brain Spine. 2023 Apr 6;3:101738. doi: 10.1016/j.bas.2023.101738. eCollection 2023. Brain Spine. 2023. PMID: 37383438 Free PMC article.
-
Burden, risk factors, neurosurgical evacuation outcomes, and predictors of mortality among traumatic brain injury patients with expansive intracranial hematomas in Uganda: a mixed methods study design.BMC Surg. 2023 Oct 25;23(1):326. doi: 10.1186/s12893-023-02227-9. BMC Surg. 2023. PMID: 37880635 Free PMC article.
References
-
- Bullock MR, Chesnut R, Ghajar J et al. . Surgical management of acute epidural hematomas. Neurosurgery. 2006;58(3 suppl):S7-S15; discussion Si-Siv Available at: http://www.ncbi.nlm.nih.gov/pubmed/16710967. Accessed March 21, 2017. - PubMed
-
- Seelig JM, Becker DP, Miller JD, Greenberg RP, Ward JD, Choi SC. Traumatic acute subdural hematoma. N Engl J Med. 1981;304(25):1511-1518. - PubMed
-
- Haselsberger K, Pucher R, Auer LM. Prognosis after acute subdural or epidural haemorrhage. Acta Neurochir. 1988;90(3-4):111-116. Available at: http://www.ncbi.nlm.nih.gov/pubmed/3354356. Accessed March 21, 2017. - PubMed
-
- Jamieson KG, Yelland JD. Extradural hematoma. Report of 167 cases. J Neurosurg. 1968;29(1):13-23. - PubMed
-
- Scotter J, Hendrickson S, Marcus HJ, Wilson MH. Prognosis of patients with bilateral fixed dilated pupils secondary to traumatic extradural or subdural haematoma who undergo surgery: a systematic review and meta-analysis. Emerg Med J. 2014:1-6. doi:10.1136/emermed-2014-204260. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
