

Arginine Metabolism Is Altered in Adults with A-β + Ketosis-Prone Diabetes
- PMID: 29490093
- PMCID: PMC6251649
- DOI: 10.1093/jn/nxx032
Arginine Metabolism Is Altered in Adults with A-β + Ketosis-Prone Diabetes
Abstract
Background: A-β + ketosis-prone diabetes (KPD) is a subset of type 2 diabetes in which patients have severe but reversible β cell dysfunction of unknown etiology. Plasma metabolomic analysis indicates that abnormal arginine metabolism may be involved.
Objective: The objective of this study was to determine the relation between gut microbiome and arginine metabolism and the relation between arginine availability and β cell function in KPD patients compared with control participants.
Methods: Kinetics of arginine and related metabolites were measured with stable isotope tracers, and insulin secretory responses to arginine and glucose were determined under euglycemic and hyperglycemic conditions in 6 KPD patients and 6 age-, gender-, and body mass index-matched control participants. Glucose potentiation of arginine-induced insulin secretion was performed in a different set of 6 KPD and 3 control participants.
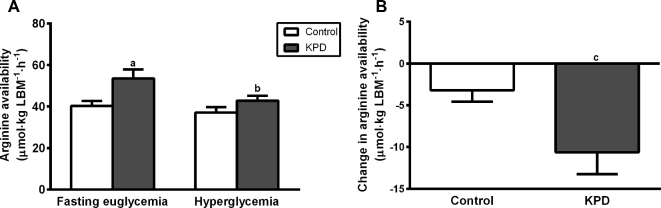
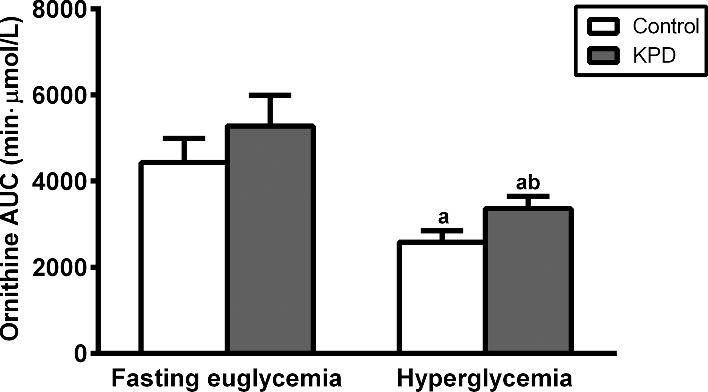
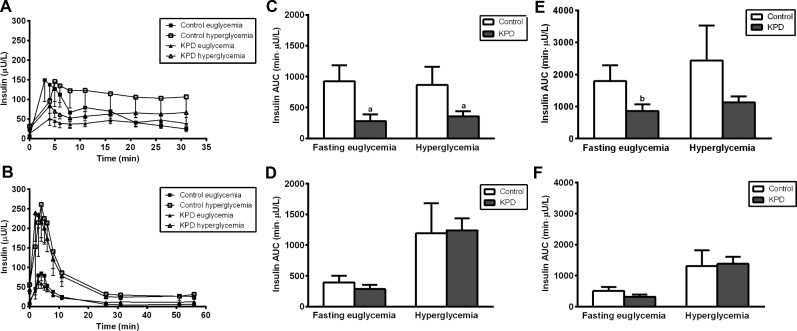
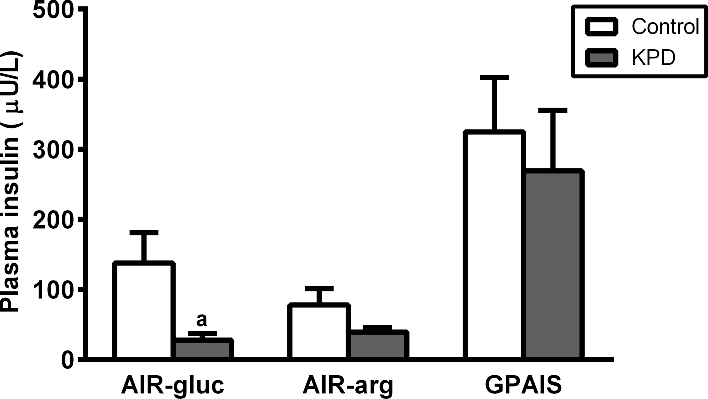
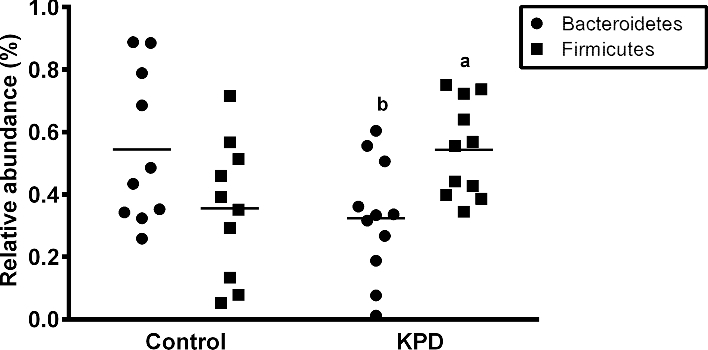
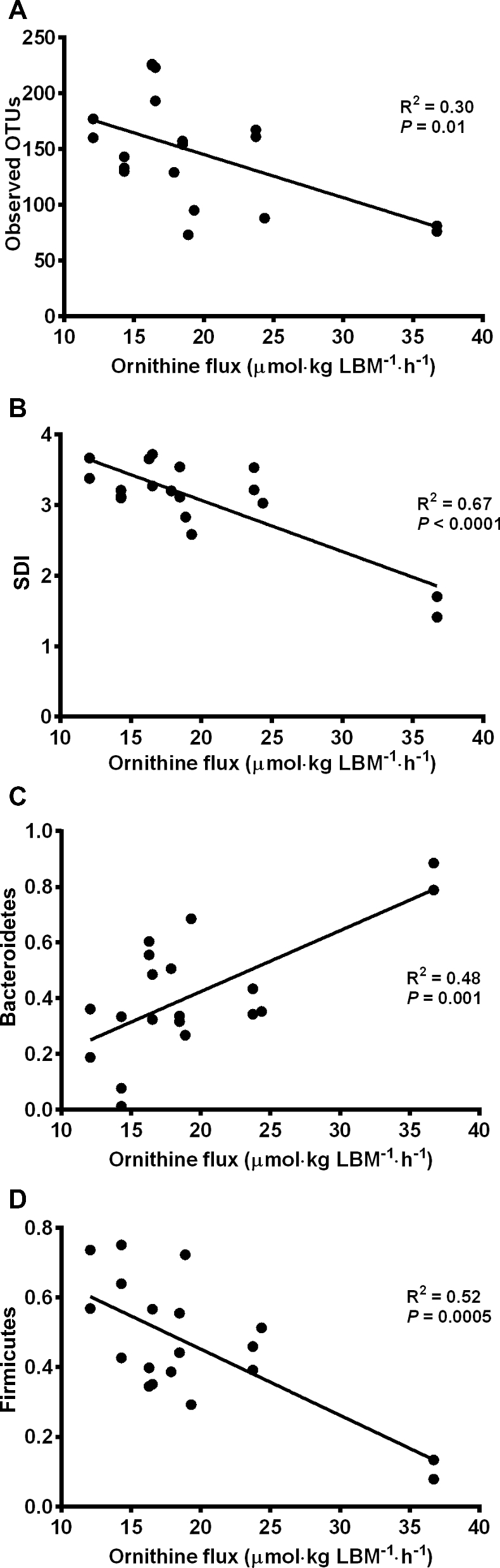
Results: Arginine availability was higher in KPD patients during euglycemia [53.5 ± 4.3 (mean ± SEM) compared with 40.3 ± 2.4 μmol · kg lean body mass (LBM)-1 · h-1, P = 0.03] but declined more in response to hyperglycemia (Δ 10.15 ± 2.6 compared with Δ 3.20 ± 1.3 μmol · kg LBM-1 · h-1, P = 0.041). During hyperglycemia, ornithine flux was not different between groups but after an arginine bolus, plasma ornithine AUC trended higher in KPD patients (3360 ± 294 compared with 2584 ± 259 min · μmol · L-1, P = 0.08). In both euglycemia and hyperglycemia, the first-phase insulin responses to glucose stimulation were lower in KPD patients (euglycemic insulin AUC 282 ± 108 compared with 926 ± 257 min · μU · mL-1, P = 0.02; hyperglycemic insulin AUC 358 ± 79 compared with 866 ± 292 min · μU · mL-1, P = 0.05), but exogenous arginine restored first-phase insulin secretion in KPD patients to the level of control participants.
Conclusion: Compared with control participants, KPD patients have increased arginine availability in the euglycemic state, indicating a higher requirement. This is compromised during hyperglycemia, with an inadequate supply of arginine to sustain metabolic functions such as insulin secretion. Exogenous arginine administration restores a normal insulin secretory response.
Figures
Comment in
-
Arginine Metabolism and A-β + Ketosis-Prone Diabetes.J Nutr. 2018 Feb 1;148(2):170-171. doi: 10.1093/jn/nxx066. J Nutr. 2018. PMID: 29490106 No abstract available.
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
