

Fast direct neuronal signaling via the IL-4 receptor as therapeutic target in neuroinflammation
- PMID: 29491183
- PMCID: PMC12102061
- DOI: 10.1126/scitranslmed.aao2304
Fast direct neuronal signaling via the IL-4 receptor as therapeutic target in neuroinflammation
Abstract
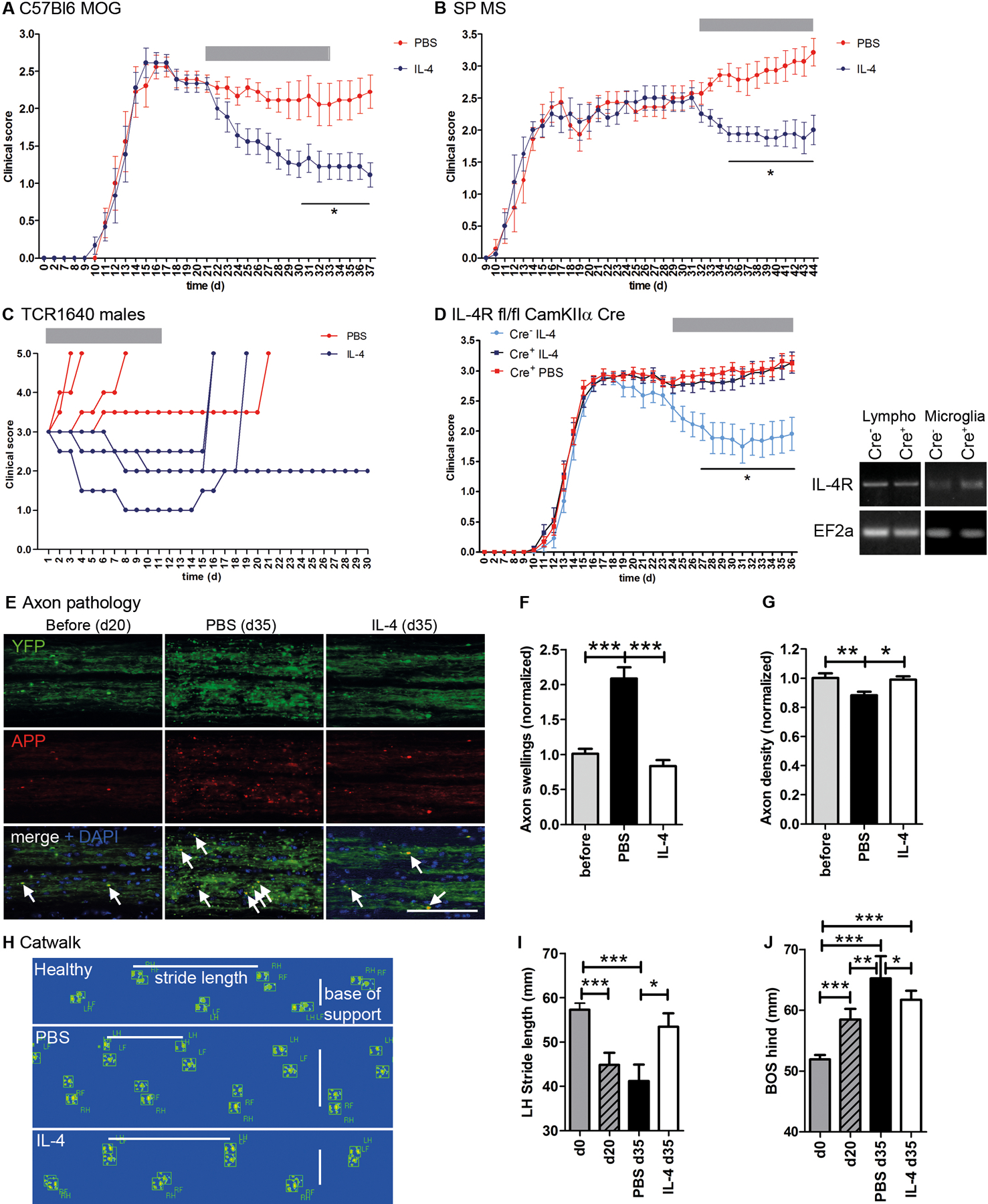
Ongoing axonal degeneration is thought to underlie disability in chronic neuroinflammation, such as multiple sclerosis (MS), especially during its progressive phase. Upon inflammatory attack, axons undergo pathological swelling, which can be reversible. Because we had evidence for beneficial effects of T helper 2 lymphocytes in experimental neurotrauma and discovered interleukin-4 receptor (IL-4R) expressed on axons in MS lesions, we aimed at unraveling the effects of IL-4 on neuroinflammatory axon injury. We demonstrate that intrathecal IL-4 treatment during the chronic phase of several experimental autoimmune encephalomyelitis models reversed disease progression without affecting inflammation. Amelioration of disability was abrogated upon neuronal deletion of IL-4R. We discovered direct neuronal signaling via the IRS1-PI3K-PKC pathway underlying cytoskeletal remodeling and axonal repair. Nasal IL-4 application, suitable for clinical translation, was equally effective in improving clinical outcome. Targeting neuronal IL-4 signaling may offer new therapeutic strategies to halt disability progression in MS and possibly also neurodegenerative conditions.
Copyright © 2018 The Authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. No claim to original U.S. Government Works.
Conflict of interest statement
Competing interests: The authors declare that they have no competing interests.
Figures






References
-
- Larochelle C, Uphaus T, Prat A, Zipp F, Secondary progression in multiple sclerosis: Neuronal exhaustion or distinct pathology? Trends Neurosci 39, 325–339 (2016). - PubMed
-
- Friese MA, Schattling B, Fugger L, Mechanisms of neurodegeneration and axonal dysfunction in multiple sclerosis. Nat. Rev. Neurol 10, 225–238 (2014). - PubMed
-
- Siffrin V, Radbruch H, Glumm R, Niesner R, Paterka M, Herz J, Leuenberger T, Lehmann SM, Luenstedt S, Rinnenthal JL, Laube G, Luche H, Lehnardt S, Fehling HJ, Griesbeck O, Zipp F, In vivo imaging of partially reversible TH17 cell-induced neuronal dysfunction in the course of encephalomyelitis. Immunity 33, 424–436 (2010). - PubMed
-
- Nikić I, Merkler D, Sorbara C, Brinkoetter M, Kreutzfeldt M, Bareyre FM, Brück W, Bishop D, Misgeld T, Kerschensteiner M, A reversible form of axon damage in experimental autoimmune encephalomyelitis and multiple sclerosis. Nat. Med 17, 495–499 (2011). - PubMed
-
- Franklin RJM, ffrench-Constant C, Edgar JM, Smith KJ, Neuroprotection and repair in multiple sclerosis. Nat. Rev. Neurol 8, 624–634 (2012). - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
