

The Anticipated Renoprotective Effects of Sodium-glucose Cotransporter 2 Inhibitors
- PMID: 29491318
- PMCID: PMC6120824
- DOI: 10.2169/internalmedicine.9842-17
The Anticipated Renoprotective Effects of Sodium-glucose Cotransporter 2 Inhibitors
Abstract
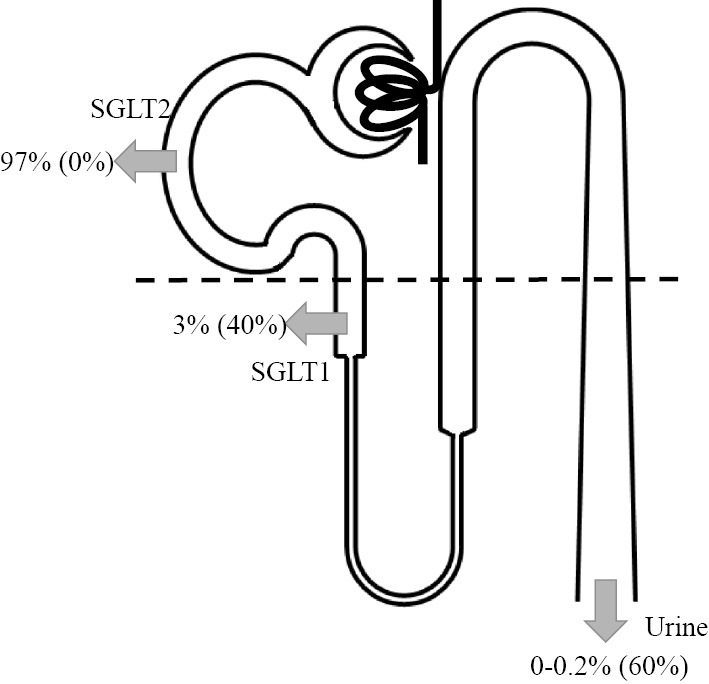
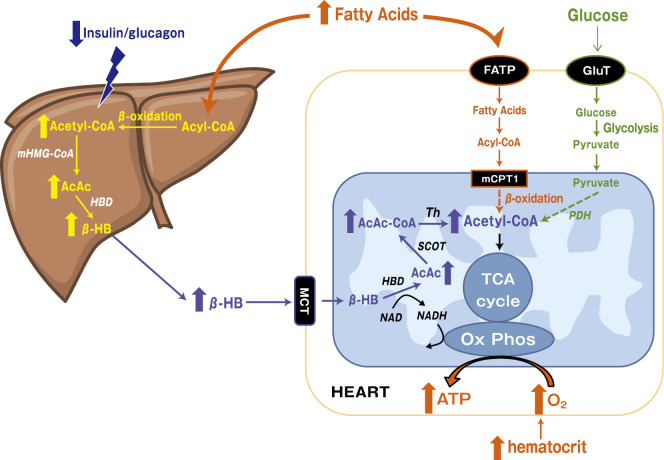
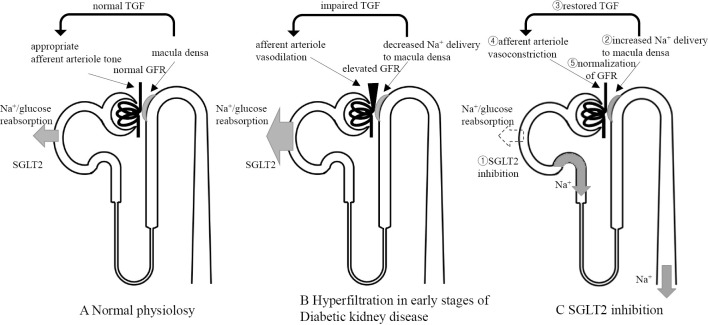
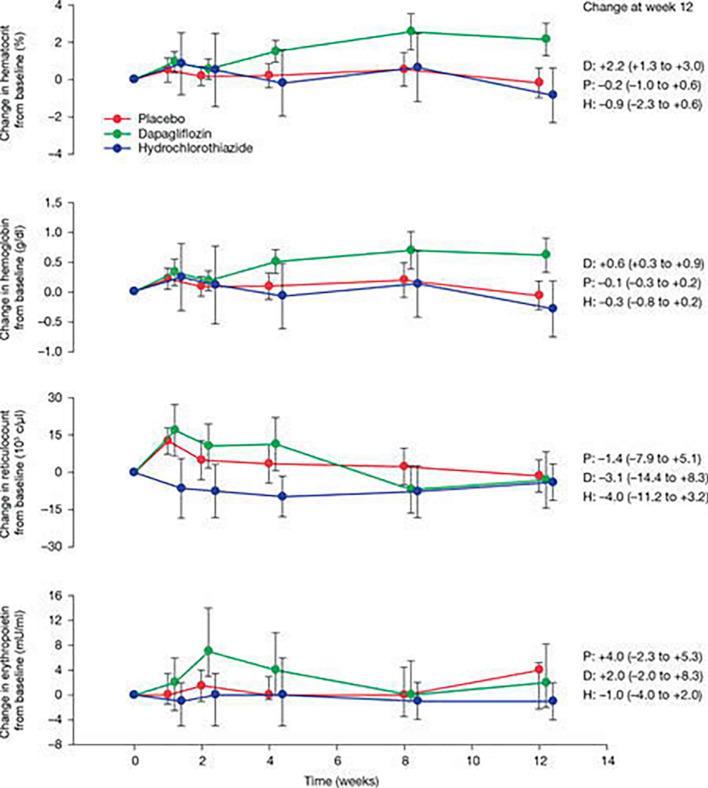
Sodium-glucose cotransporter 2 (SGLT2), which is specifically expressed on the apical side of proximal tubular cells, is involved in the reabsorption of most of the glucose filtered by the glomeruli, and its inhibitors are gaining publicity as potent antihyperglycemic drugs. In some clinical trials, SGLT2 inhibitors exerted cardiovascular and kidney protective effects, which appeared to be partly independent of the original glucose-lowering effect. SGLT2 inhibitors have both direct and indirect renoprotective effects. The direct effects involve the suppression of hyperplasia/hypertrophy, inflammation, and fibrosis in the proximal tubular cells, utilization of ketone bodies, restored tubuloglomerular feedback, decreased oxygen consumption, improvement in anemia, and preconditioning against ischemia/reperfusion. The indirect effects involve a reduction in insulin levels and resistance, uric acid concentration, body weight, and blood pressure. However, safety concerns remain, including consequences of an enhanced glucose load in the lower nephron, leg amputation, bone fractures, and therapeutic efficacy in patients with advanced chronic kidney disease.
Keywords: diabetic kidney disease; final common pathway; sodium-glucose cotransporter 2 (SGLT2) inhibitors; tubuloglomerular feedback (TGF).
Figures
References
-
- Škrtić M, Cherney DZI. Sodium-glucose cotransporter-2 inhibition and the potential for renal protection in diabetic nephropathy. Curr Opin Nephrol Hypertens 24: 96-103, 2015. - PubMed
-
- Zinman B, Wanner C, Lachin JM, Fitchett D, Bluhmki E, Hantel S, et al. . Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med 373: 2117-2128, 2015. - PubMed
-
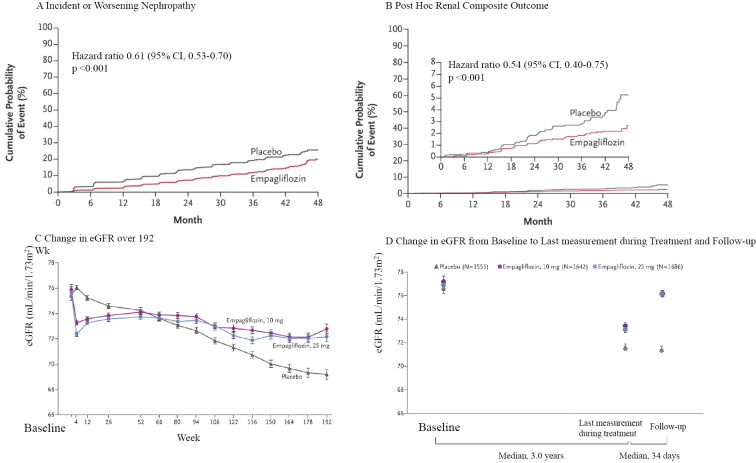
- Wanner C, Inzucchi SE, Lachin JM, et al. . Empagliflozin and progression of kidney disease in type 2 diabetes. N Engl J Med 375: 323-334, 2016. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical