

Ruptured hepatic aneurysm as first presenting symptom of polyarteritis nodosa
- PMID: 29492271
- PMCID: PMC5822702
- DOI: 10.1093/omcr/omx100
Ruptured hepatic aneurysm as first presenting symptom of polyarteritis nodosa
Abstract
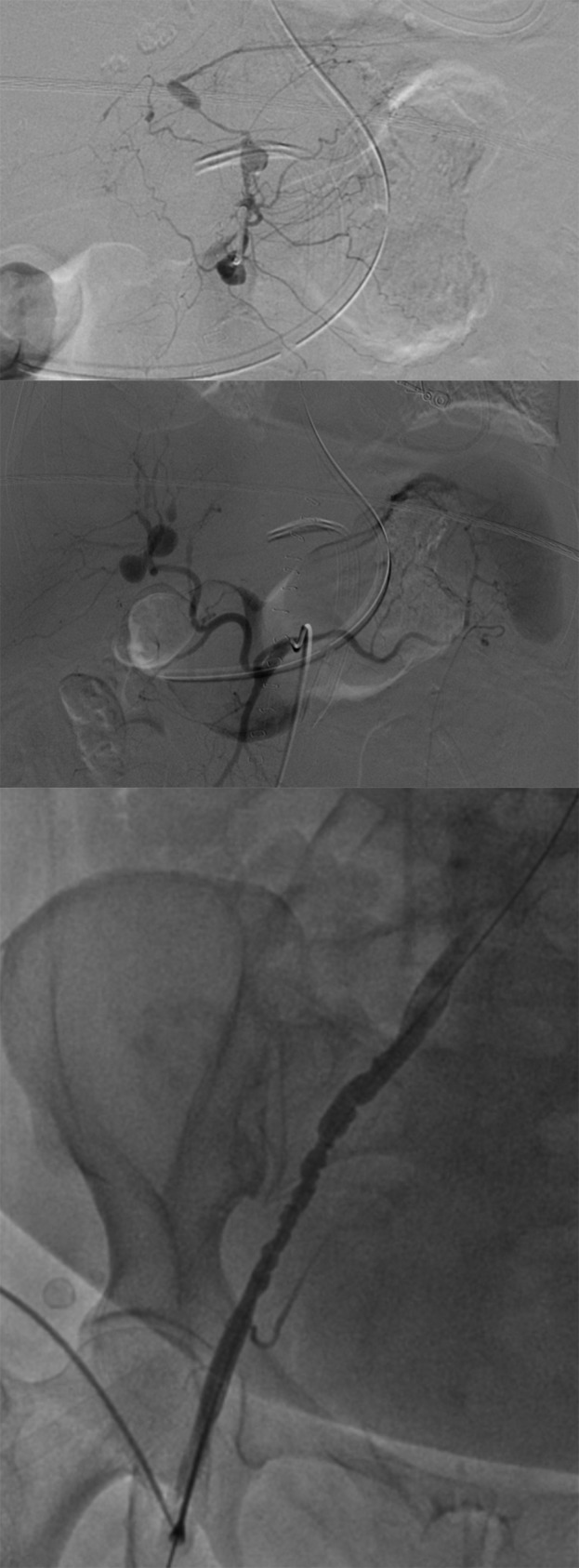
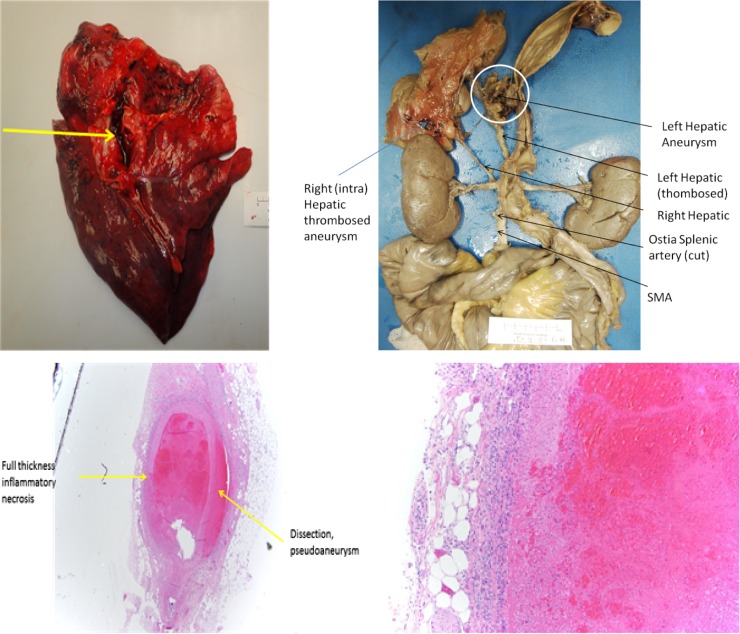
Polyarteritis nodosa (PAN) is an inflammatory vasculitis that creates regions of stenosis and aneurysm formation. The authors describe a 66-year-old female with hepatic artery rupture as the first presentation of undiagnosed PAN, presenting with abdominal pain followed by hemorrhagic shock. This aneurysm was suture ligated with a successful outcome. A mesenteric arteriogram demonstrated lesions consistent with PAN including aneurysms of the left gastric branches, right and left hepatic arteries, and beaded appearance of the iliac artery. However, she developed massive pulmonary embolism from which she did not recover after discharge. Postmortem examination confirmed left hepatic artery aneurysm rupture and changes consistent with PAN on gross anatomical examination and histology. This report provides a unique overview of the disease process through imaging, gross anatomic specimen and pathology. Life-threatening hepatic artery aneurysm rupture is an uncommon presentation of PAN which may benefit readers in creating a more robust differential diagnosis.
Figures

References
-
- Balow JE. Renal vasculitis. Kidney Int 1985;27:954. - PubMed
-
- Sato O, Cohn DL. Polyarteritis and microscopic polyangiitis In: Klippel JH, Dieppe PA, eds.. Rheumatology. St Louis: Mosby, 2003, 1290–99.
-
- Kallenberg CG, Brouwer E, Weening JJ, Tervaert JW. Anti-neutrophil cytoplasmic antibodies: current diagnostic and pathophysiological potential. Kidney Int 1994;46:1. - PubMed
-
- Lightfoot RW Jr, Michel BA, Bloch DA, Hunder GG, Zvaifler NJ, McShane DJ, et al. The American College of Rheumatology 1990 criteria for the classification of polyarteritisnodosa. Arthritis Rheum 1990;33:1088. - PubMed
-
- Travers RL, Allison DJ, Brettie RP, Hughes GR. Polyarteritisnodosa: a clinical and angiographic analysis of 17 cases. Semin Arthritis Rheum 1979;8:184–99. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
