

Computed tomography findings after radiofrequency ablation in locally advanced pancreatic cancer
- PMID: 29492602
- PMCID: PMC6132871
- DOI: 10.1007/s00261-018-1519-y
Computed tomography findings after radiofrequency ablation in locally advanced pancreatic cancer
Abstract
Purpose: The purpose of the study was to provide a systematic evaluation of the computed tomography(CT) findings after radiofrequency ablation (RFA) in locally advanced pancreatic cancer(LAPC).
Methods: Eighteen patients with intra-operative RFA-treated LAPC were included in a prospective case series. All CT-scans performed prior to RFA and 1 week and 3 months of post-RFA, according to standard regimen, were assessed by two radiologists in consensus, using standardized radiological scoring lists.
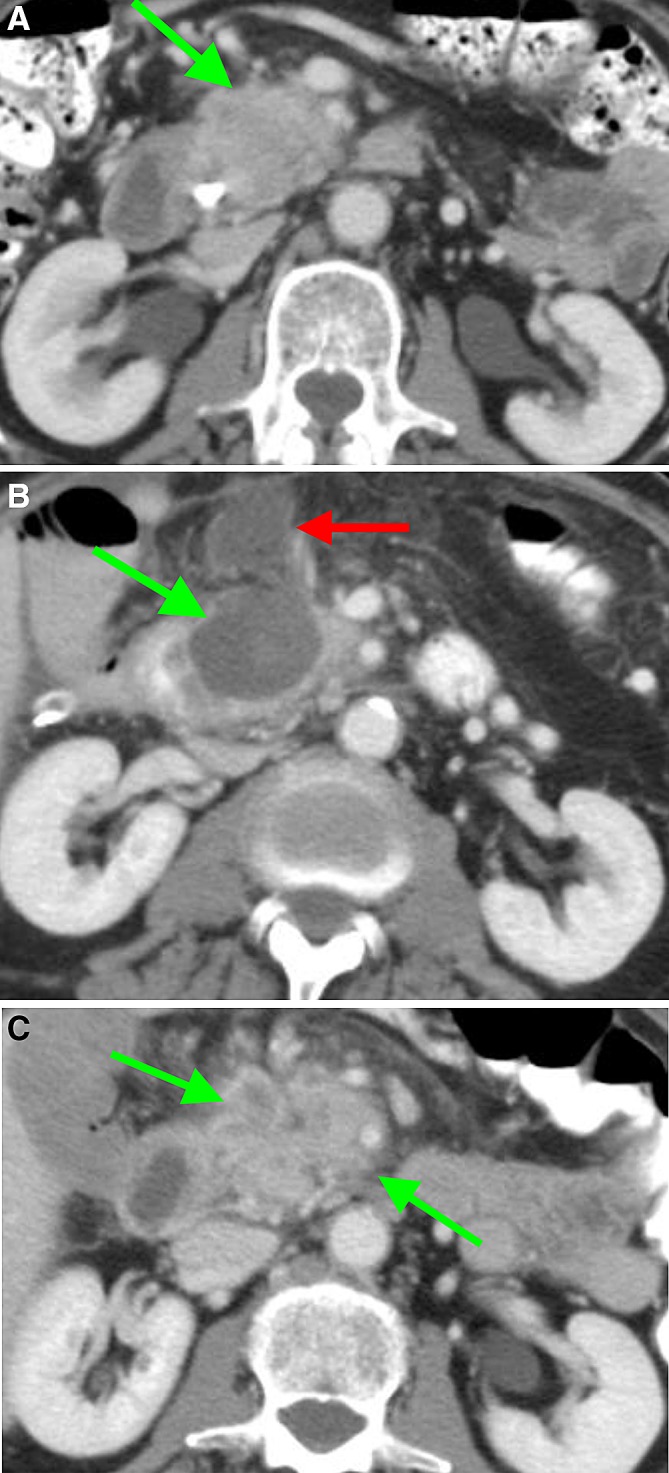
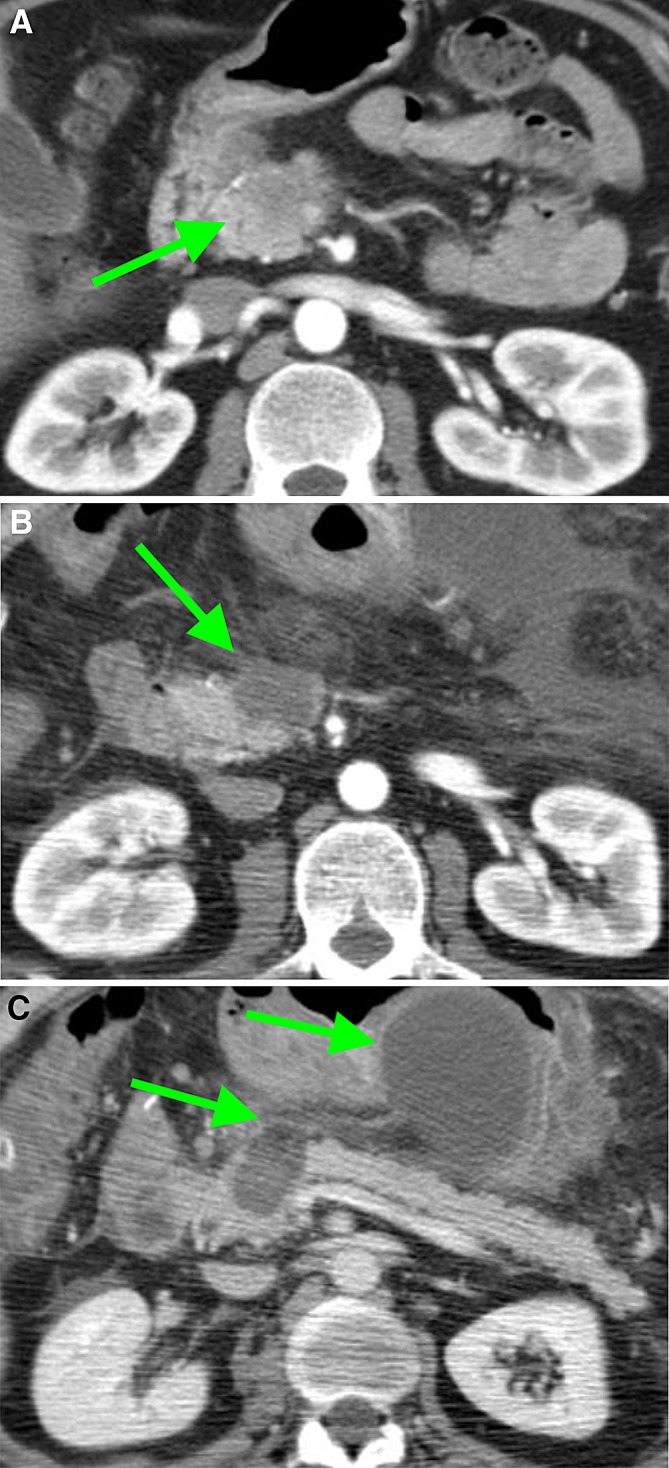
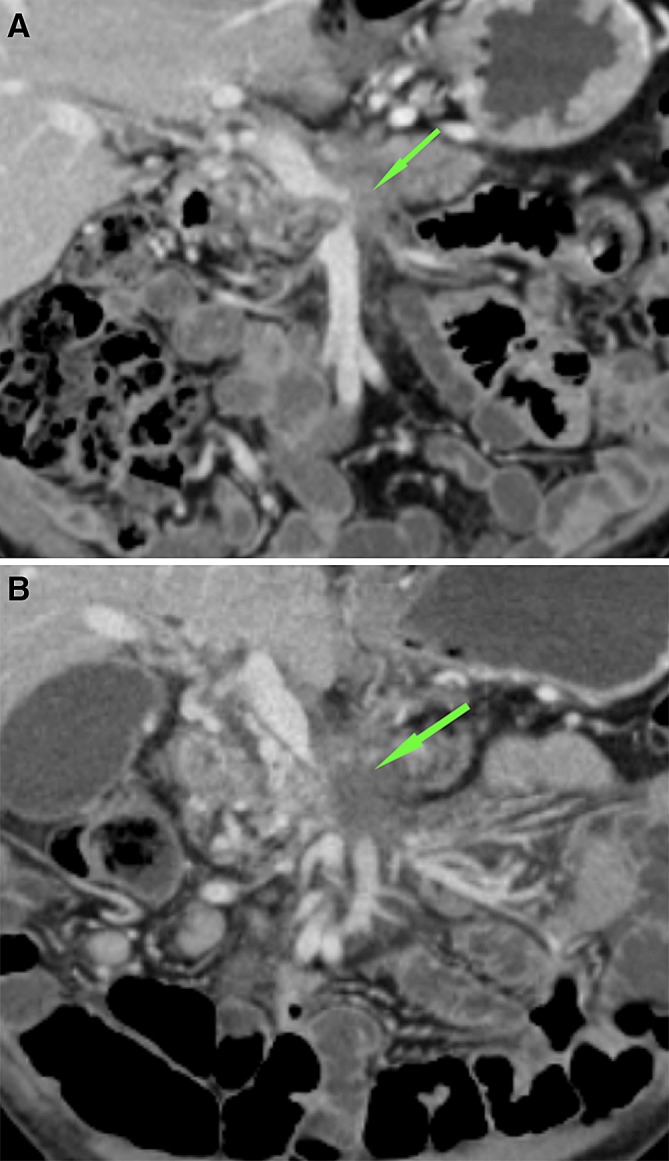
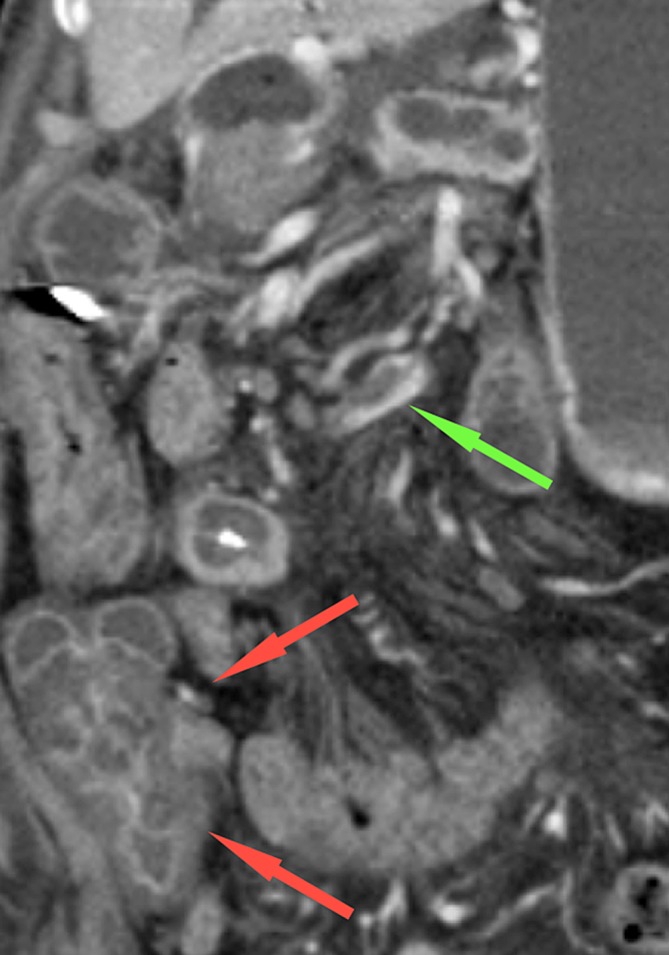
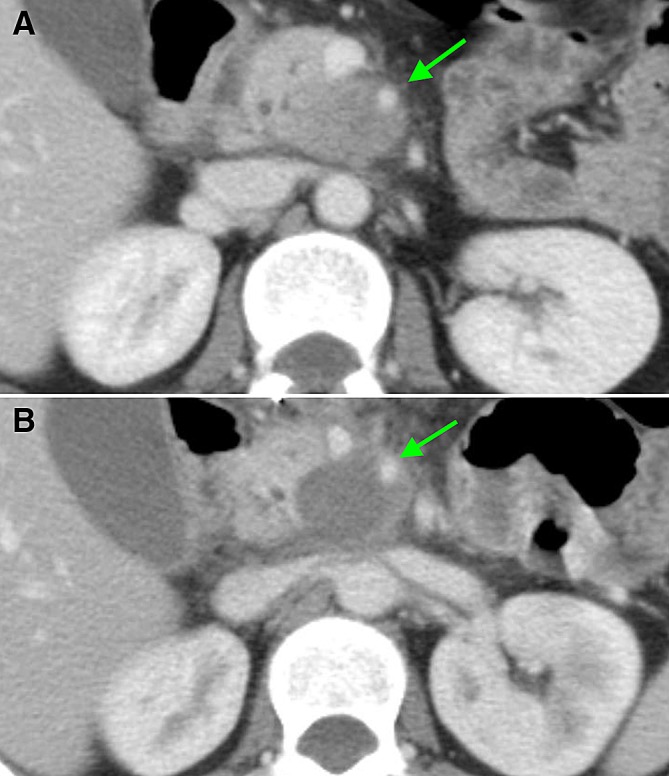
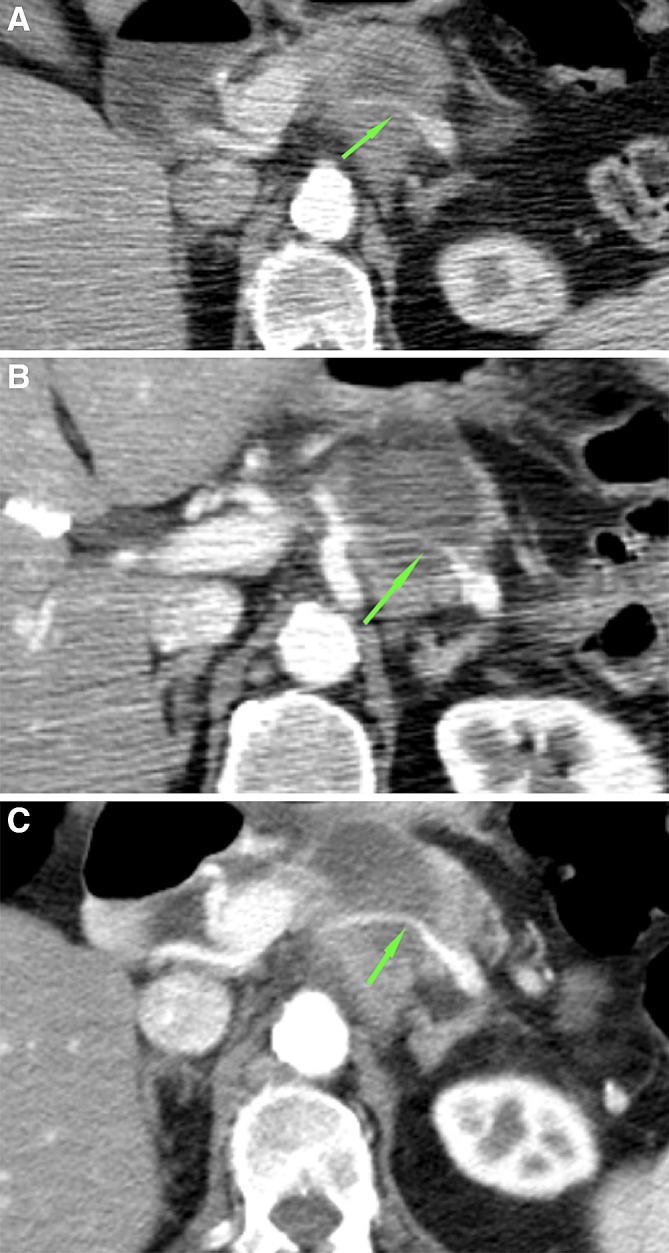
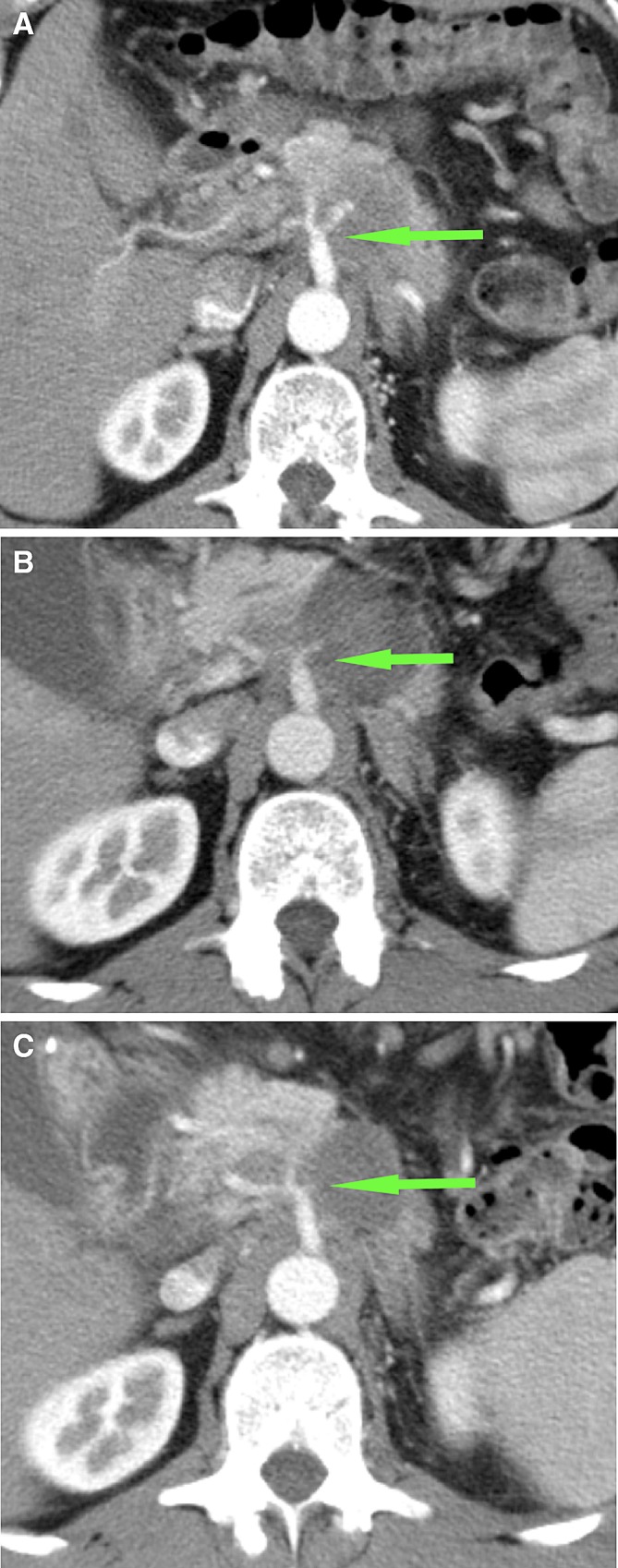
Results: 51 CT-scans were assessed. One week after RFA, the ablation zone was visible in all patients as a (partially) sharply defined (83%), heterogeneous area (94%). At 3 months of follow-up, the ablation zone was completely invaded by tumor in 67% of patients and still present, but decreased in 33%. In two patients (11%), local thrombosis and/or occlusion of the superior mesenteric vein occurred. The occlusions persisted without clinical consequences and the thrombosis disappeared. A peripancreatic fluid collection was visible 1 week after RFA in 3 patients, wherein the ablation zone extended ventrally outside of the pancreas.
Conclusions: Directly after RFA for LAPC, a well-defined ablation zone is visible on CT-imaging. This ablation zone is usually replaced by tumor ingrowth after 3 months. Moreover, the ablation zone regularly included vascular structures, with rare asymptomatic venous occlusion or thrombosis and without adverse effects on arteries.
Keywords: Computed tomography; Imaging findings; Locally advanced pancreatic cancer; Radiofrequency ablation.
Conflict of interest statement
All the authors declare that they have no conflict of interest.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
