

The 2014 updated version of the Confusion Assessment Method for the Intensive Care Unit compared to the 5th version of the Diagnostic and Statistical Manual of Mental Disorders and other current methods used by intensivists
- PMID: 29492696
- PMCID: PMC5833335
- DOI: 10.1186/s13613-018-0377-7
The 2014 updated version of the Confusion Assessment Method for the Intensive Care Unit compared to the 5th version of the Diagnostic and Statistical Manual of Mental Disorders and other current methods used by intensivists
Abstract
Background: One third of patients admitted to an intensive care unit (ICU) will develop delirium. However, delirium is under-recognized by bedside clinicians without the use of delirium screening tools, such as the Intensive Care Delirium Screening Checklist (ICDSC) or the Confusion Assessment Method for the ICU (CAM-ICU). The CAM-ICU was updated in 2014 to improve its use by clinicians throughout the world. It has never been validated compared to the new reference standard, the Diagnostic and Statistical Manual of Mental Disorders 5th version (DSM-5).
Methods: We made a prospective psychometric study in a 16-bed medical-surgical ICU of a French academic hospital, to measure the diagnostic performance of the 2014 updated CAM-ICU compared to the DSM-5 as the reference standard. We included consecutive adult patients with a Richmond Agitation Sedation Scale (RASS) ≥ -3, without preexisting cognitive disorders, psychosis or cerebral injury. Delirium was independently assessed by neuropsychological experts using an operationalized approach to DSM-5, by investigators using the CAM-ICU and the ICDSC, by bedside clinicians and by ICU patients. The sensitivity, specificity, positive and negative predictive values were calculated considering neuropsychologist DSM-5 assessments as the reference standard (primary endpoint). CAM-ICU inter-observer agreement, as well as that between delirium diagnosis methods and the reference standard, was summarized using κ coefficients, which were subsequently compared using the Z-test.
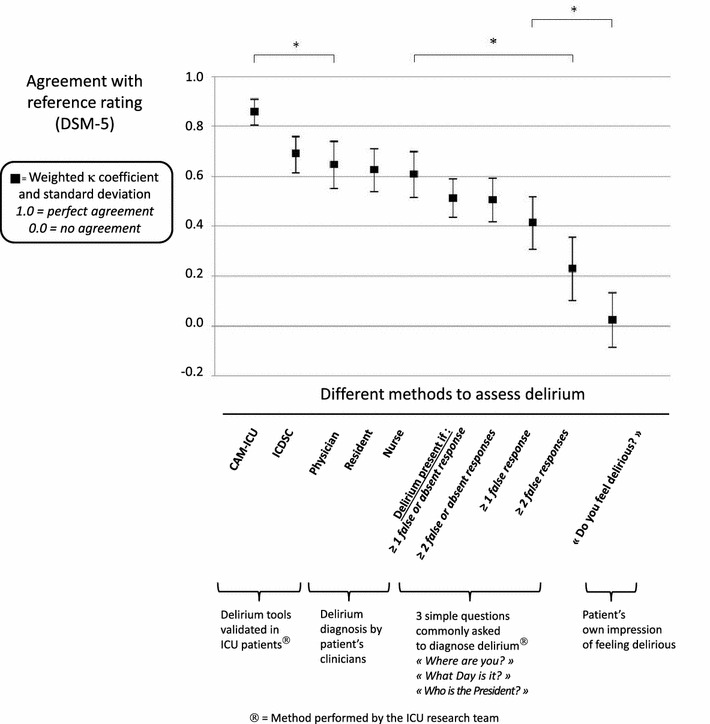
Results: Delirium was diagnosed by experts in 38% of the 108 patients included for analysis. The CAM-ICU had a sensitivity of 83%, a specificity of 100%, a positive predictive value of 100% and a negative predictive value of 91%. Compared to the reference standard, the CAM-ICU had a significantly (p < 0.05) higher agreement (κ = 0.86 ± 0.05) than the physicians,' residents' and nurses' diagnoses (κ = 0.65 ± 0.09; 0.63 ± 0.09; 0.61 ± 0.09, respectively), as well as the patient's own impression of feeling delirious (κ = 0.02 ± 0.11). Differences between the ICDSC (κ = 0.69 ± 0.07) and CAM-ICU were not significant (p = 0.054). The CAM-ICU demonstrated a high reliability for inter-observer agreement (κ = 0.87 ± 0.06).
Conclusions: The 2014 updated version of the CAM-ICU is valid according to DSM-5 criteria and reliable regarding inter-observer agreement in a research setting. Delirium remains under-recognized by bedside clinicians.
Keywords: Critical care; Delirium; Intensive care unit.
Figures

References
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
