

Increased healthcare utilization associated with complete atrioventricular block in pacemaker patients
- PMID: 29492807
- PMCID: PMC5902523
- DOI: 10.1007/s10840-018-0336-0
Increased healthcare utilization associated with complete atrioventricular block in pacemaker patients
Abstract
Purpose: The purpose of the current study is to characterize and quantify the impact of complete atrioventricular block (cAVB) on heart failure hospitalization (HFH) and healthcare utilization in pacemaker (PM) patients.
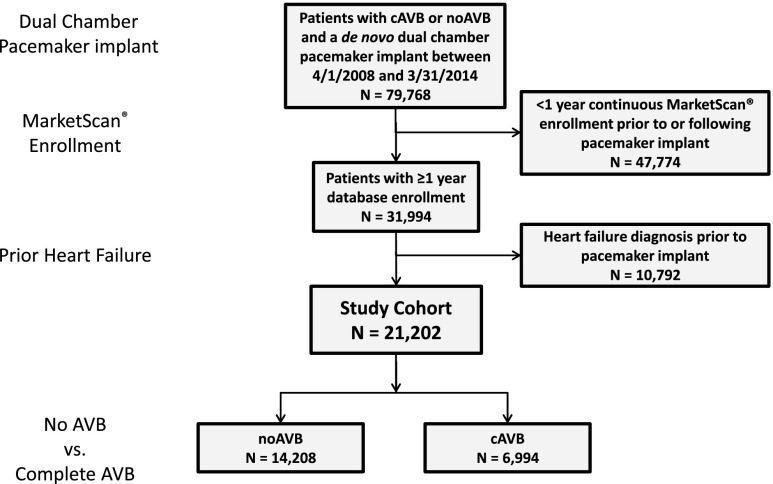
Methods: Patients ≥ 18 years implanted with a dual-chamber PM from April 2008 to March 2014 were selected from the MarketScan® Commercial and Medicare Supplemental claims databases. Patients with ≤ 1-year continuous MarketScan enrollment prior to and post-implant, and those with prior HF diagnosis were excluded. Patients were dichotomized into those with cAVB, defined as a 3rd degree AVB diagnosis or AV node ablation in the year prior to PM implant, versus those without any AVB (noAVB). Post-implant HFH and associated costs were compared based on inpatient claims.
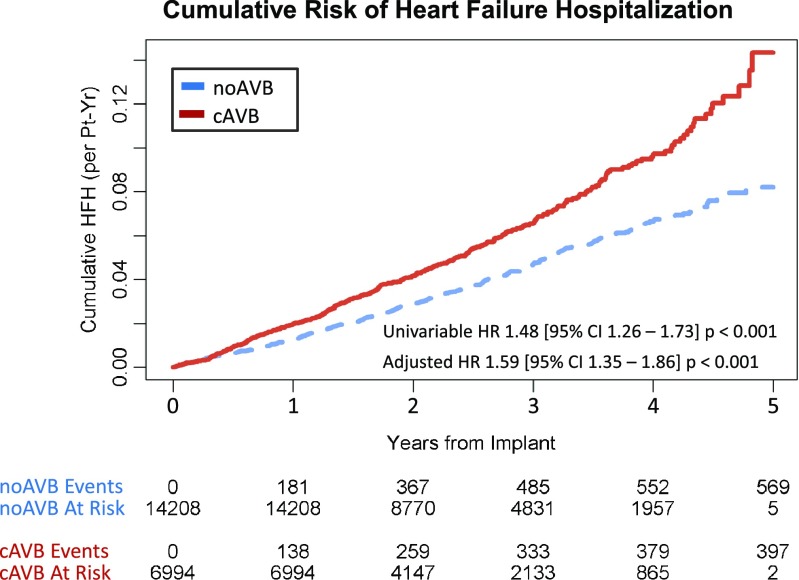
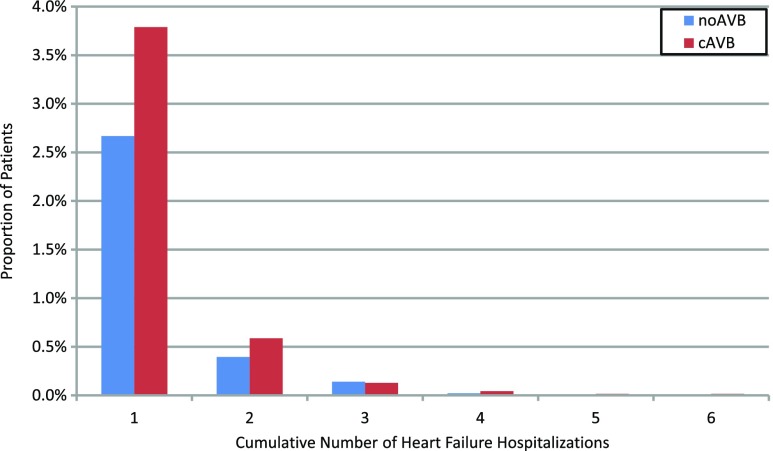
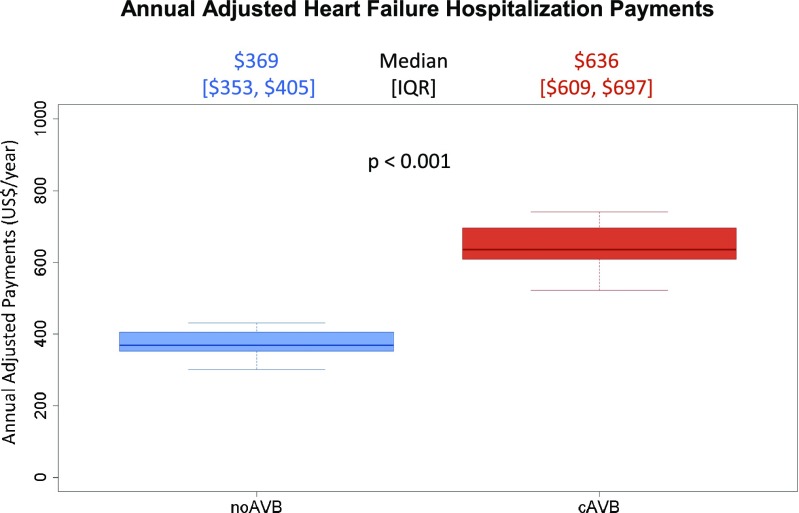
Results: The study cohort included 21,202 patients, of which 14,208 had no AVB and 6994 had cAVB, followed for 2.39 and 2.27 years, respectively. Patients with cAVB were associated with a significantly increased risk of cumulative HFH (HR 1.59 [95% CI 1.35-1.86] p < 0.001) and significantly higher costs ($636 [609-697] vs $369 [353-405] per pt-year, p < 0.001) compared to those with no AVB.
Conclusions: Among dual-chamber PM patients without prior HF, cAVB is associated with a significantly increased risk of HFH and greater HF-related healthcare utilization. Identifying patients at high risk for HF in the setting of RV pacing, and potentially earlier use of biventricular or selective conduction system pacing, may reduce HF-related healthcare utilization.
Keywords: Atrioventricular block; Healthcare utilization; Heart failure; Pacemakers; Right ventricular pacing.
Conflict of interest statement
SM: Consulting fees from Abbott.
DLM: None.
MHH: Consulting fees from Abbott.
JBP: Stock Medtronic, Inc., stock and salary from Abbott.
GJR: Stock and salary from Abbott.
YN: Stock and salary from Abbott.
FMM: None.
Figures
References
-
- Ebert M, Jander N, Minners J, Blum T, Doering M, Bollmann A, Hindricks G, Arentz T, Kalusche D, Richter S. Long-term impact of right ventricular pacing on left ventricular systolic function in pacemaker recipients with preserved ejection fraction: results from a large single-center registry. J Am Heart Assoc. 2016;5(7):e003485. doi: 10.1161/JAHA.116.003485. - DOI - PMC - PubMed
-
- Kiehl EL, Makki T, Kumar R, Gumber D, Kwon DH, Rickard JW, Kanj M, Wazni OM, Saliba WI, Varma N, Wilkoff BL, Cantillon DJ. Incidence and predictors of right ventricular pacing-induced cardiomyopathy in patients with complete atrioventricular block and preserved left ventricular systolic function. Heart Rhythm. 2016;13(12):2272–2278. doi: 10.1016/j.hrthm.2016.09.027. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
