

Disease Management plus Recommended Care versus Recommended Care Alone for Ambulatory Patients with Chronic Obstructive Pulmonary Disease
- PMID: 29494211
- PMCID: PMC6009010
- DOI: 10.1164/rccm.201711-2182OC
Disease Management plus Recommended Care versus Recommended Care Alone for Ambulatory Patients with Chronic Obstructive Pulmonary Disease
Abstract
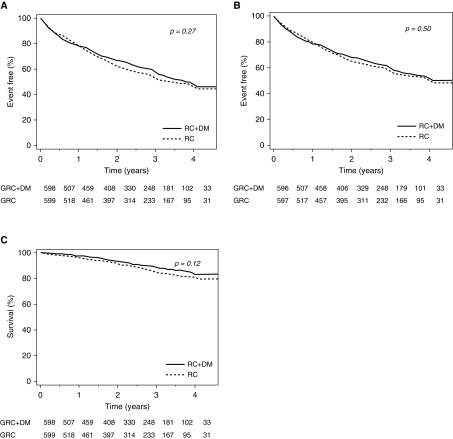
Rationale: The efficacy of disease management programs in the treatment of patients with chronic obstructive pulmonary disease (COPD) remains uncertain.Objectives: To study the effect of disease management (DM) added to recommended care (RC) in ambulatory patients with COPD.Measurements and Main Results: In this trial, 1,202 patients with COPD (age, ≥40 yr), with moderate to very severe airflow limitation were randomly assigned either to DM plus RC (study intervention) or to RC alone (control intervention). RC included follow-up by pulmonologists, inhaled long-acting bronchodilators and corticosteroids, smoking cessation intervention, nutritional advice and psychosocial support when indicated, and supervised physical activity sessions. DM, delivered by trained nurses during patients' visits to the designated COPD centers and by remote contacts with the patients between these visits, included patient self-care education, monitoring patients' symptoms and adherence to treatment, provision of advice in case of acute disease exacerbation, and coordination of care vis-à-vis other healthcare providers. The primary composite endpoint was first hospital admission for respiratory symptoms or death from any cause. During 3,537 patient-years, 284 patients (47.2%) in the control group and 264 (44.0%) in the study intervention group had a primary endpoint event. The median (range) time elapsed until a primary endpoint event was 1.0 (0-4.0) years among patients assigned to the study intervention and 1.1 (0-4.1) years among patients assigned to the control intervention; adjusted hazard ratio, 0.92 (95% confidence interval, 0.77-1.08).Conclusions: DM added to RC was not superior to RC alone in delaying first hospital admission or death among ambulatory patients with COPD.
Keywords: chronic obstructive pulmonary disease; disease management; hospitalization(s); mortality; pulmonary rehabilitation.
Figures

References
-
- Buist AS, McBurnie MA, Vollmer WM, Gillespie S, Burney P, Mannino DM, et al. BOLD Collaborative Research Group. International variation in the prevalence of COPD (the BOLD Study): a population-based prevalence study. Lancet. 2007;370:741–750. - PubMed
-
- World Health Organization. The top 10 causes of death. Geneva, Switzerland: World Health Organization; 2017 [accessed 2017 Mar 1]. Available from: http://www.who.int/mediacentre/factsheets/fs310/en/
LinkOut - more resources
Full Text Sources
Other Literature Sources
