

Causes of death and early life determinants of survival in homozygous sickle cell disease: The Jamaican cohort study from birth
- PMID: 29494636
- PMCID: PMC5832208
- DOI: 10.1371/journal.pone.0192710
Causes of death and early life determinants of survival in homozygous sickle cell disease: The Jamaican cohort study from birth
Abstract
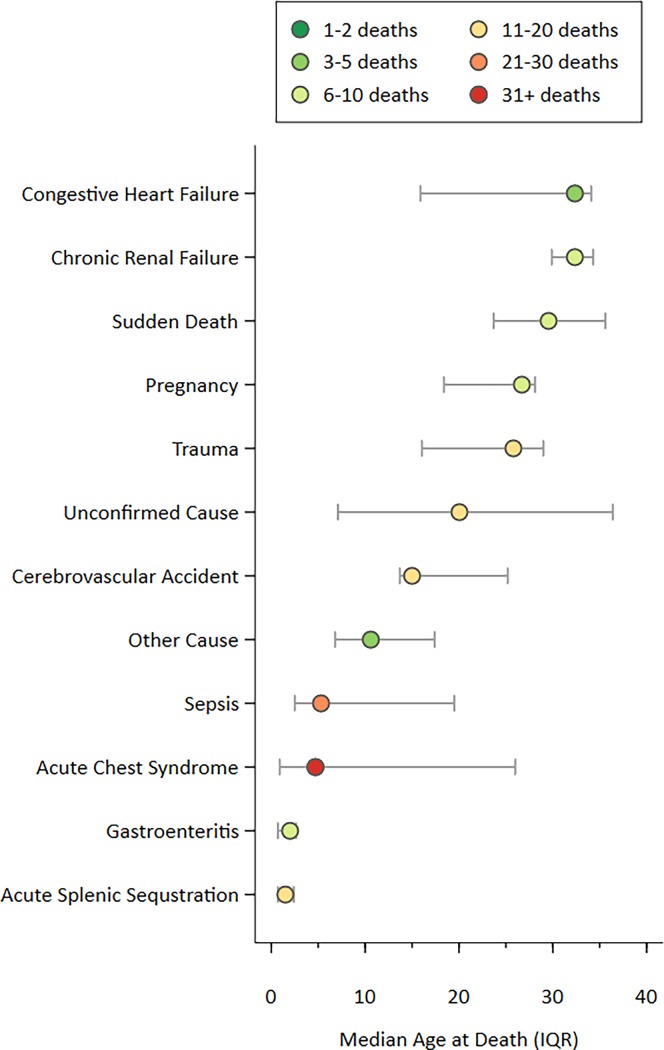
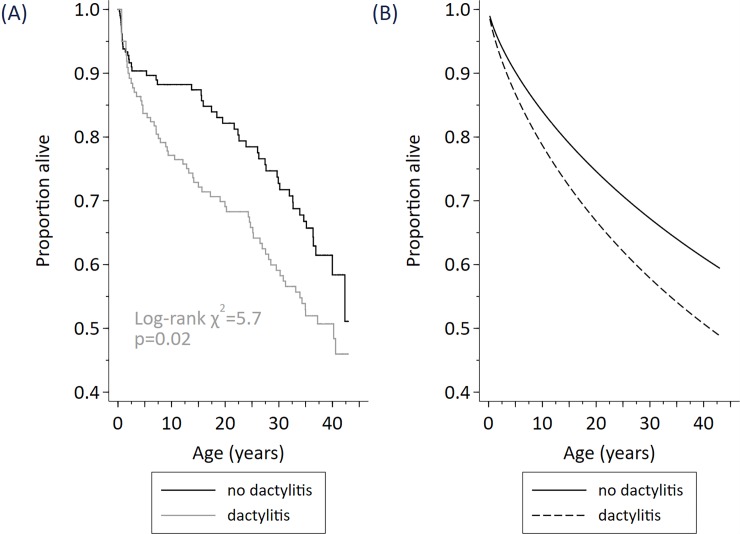
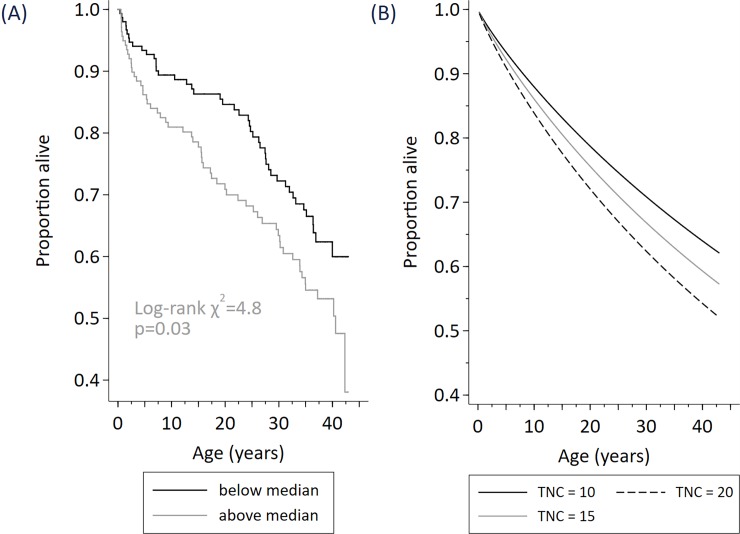
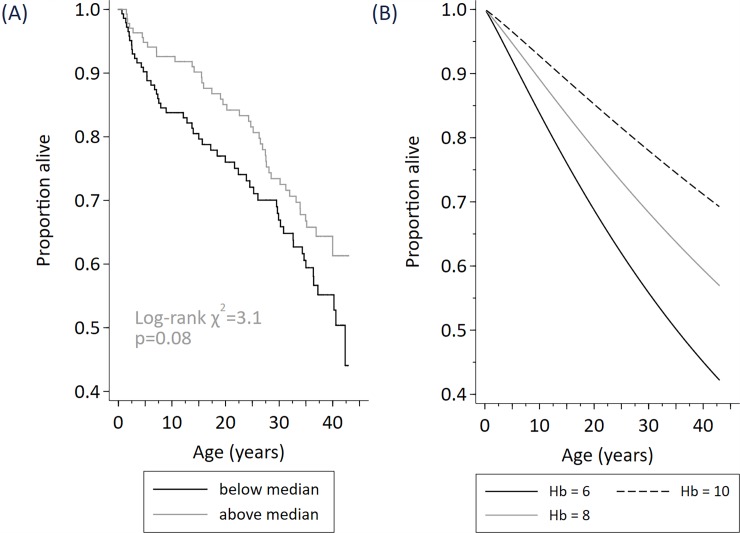
Globally, the majority of persons born with sickle cell disease do not have access to hydroxyurea or more expensive interventions. The objectives were to estimate the survival in homozygous sickle cell disease, unbiased by symptomatic selection and to ascertain the causes of death in a pre-hydroxyurea population. The utility of early life biomarkers and genetically determined phenotypes to predict survival was assessed. A cohort study based on neonatal diagnosis was undertaken at the Sickle Cell Unit, a specialist clinic delivering care to persons with sickle cell disease in Jamaica. Screening of 100,000 deliveries detected 315 babies with homozygous sickle cell disease of whom 311 have been followed from birth for periods up to 43 years. Pneumococcal prophylaxis and teaching mothers splenic palpation were important, inexpensive interventions. Anticipatory guidance, routine care and out-patient acute care were provided. Each participant was classified as alive, dead, or defaulted (usually emigration). Causes of death were ascertained from clinical records and/or post-mortem reports. Survival was assessed using the Kaplan-Meier function. Sex-adjusted Cox semi-parametric proportional hazards and Weibull modelling were used to assess the effects on survival of biomarkers. Survival to 40 years was 55.5% (95% CI 48.7% to 61.7%). Acute Chest Syndrome (n = 31) and septicemia (n = 14) were significant causes of death at all ages. Acute splenic sequestration (n = 12) was the most common cause of early deaths. Survival was significantly shorter in those with lower hemoglobin at 1 year, high total nucleated count at 1 year, and a history of dactylitis ever. In these hydroxyurea naïve patients, survival into midlife was common. Causes of death were often age specific and some may be preventable. Early life biomarkers predictive of decreased survival in SS disease identify a patient group likely to benefit from close clinical supervision and potentially high risk therapies.
Conflict of interest statement
Figures
References
-
- Platt OS, Brambilla DJ, Rosse WF, Milner PF, Castro O, Steinberg MH, et al. (1994) Mortality in sickle cell disease. Life expectancy and risk factors for early death. N Engl J Med 330: 1639–1644. doi: 10.1056/NEJM199406093302303 - DOI - PubMed
-
- Wierenga KJ, Hambleton IR, Lewis NA (2001) Survival estimates for patients with homozygous sickle-cell disease in Jamaica: a clinic-based population study. Lancet 357: 680–683. - PubMed
-
- Serjeant GR, Serjeant BE, Forbes M, Hayes RJ, Higgs DR, Lehmann H (1986) Haemoglobin gene frequencies in the Jamaican population: a study in 100,000 newborns. Br J Haematol 64: 253–262. - PubMed
-
- Miller ST, Sleeper LA, Pegelow CH, Enos LE, Wang WC, Weiner SJ, et al. (2000) Prediction of adverse outcomes in children with sickle cell disease. N Engl J Med 342: 83–89. doi: 10.1056/NEJM200001133420203 - DOI - PubMed
-
- Mears JG, Lachman HM, Labie D, Nagel RL (1983) Alpha-thalassemia is related to prolonged survival in sickle cell anemia. Blood 62: 286–290. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
