

Is Textbook Outcome a valuable composite measure for short-term outcomes of gastrointestinal treatments in the Netherlands using hospital information system data? A retrospective cohort study
- PMID: 29496668
- PMCID: PMC5855341
- DOI: 10.1136/bmjopen-2017-019405
Is Textbook Outcome a valuable composite measure for short-term outcomes of gastrointestinal treatments in the Netherlands using hospital information system data? A retrospective cohort study
Abstract
Objective: To develop a feasible model for monitoring short-term outcome of clinical care trajectories for hospitals in the Netherlands using data obtained from hospital information systems for identifying hospital variation.
Study design: Retrospective analysis of collected data from hospital information systems combined with clinical indicator definitions to define and compare short-term outcomes for three gastrointestinal pathways using the concept of Textbook Outcome.
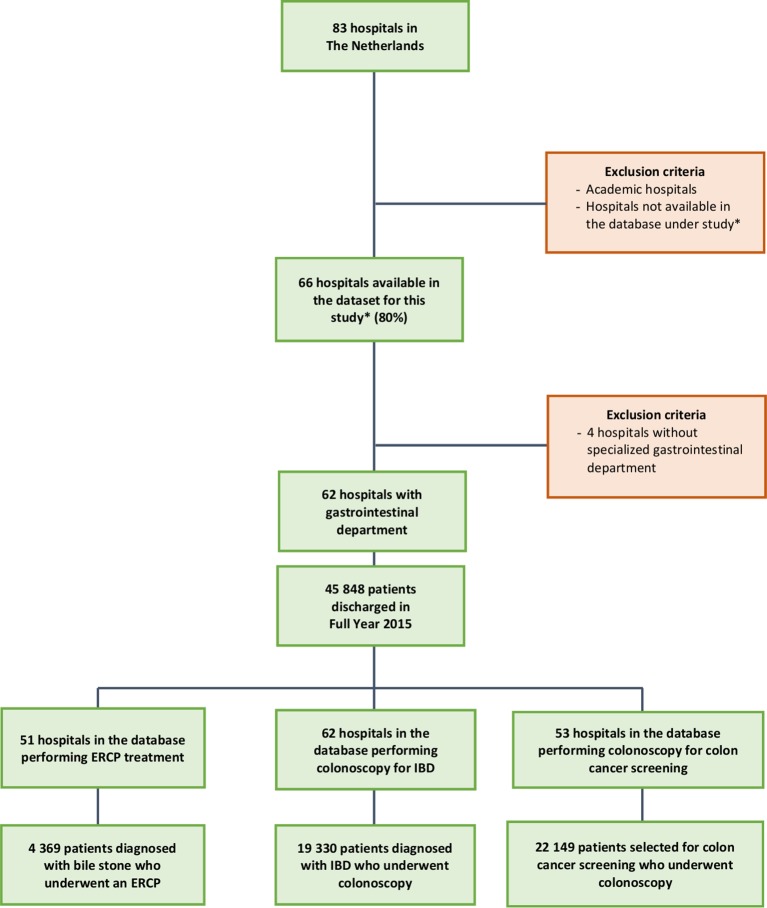
Setting: 62 Dutch hospitals.
Participants: 45 848 unique gastrointestinal patients discharged in 2015.
Main outcome measure: A broad range of clinical outcomes including length of stay, reintervention, readmission and doctor-patient counselling.
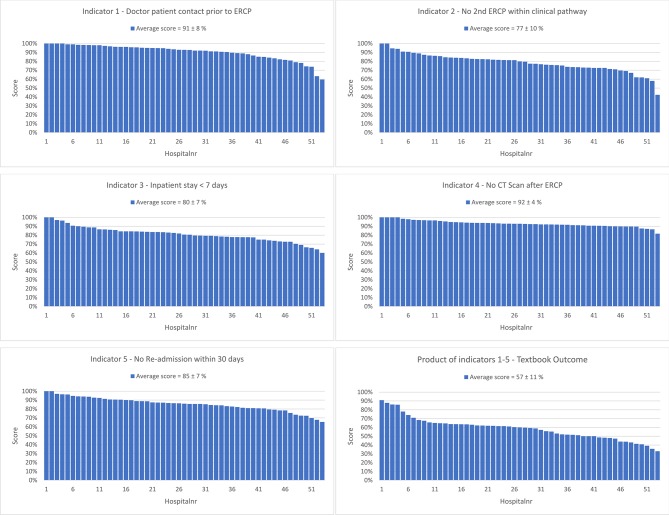
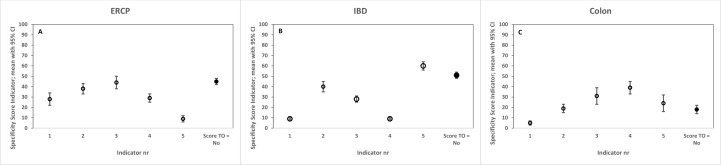
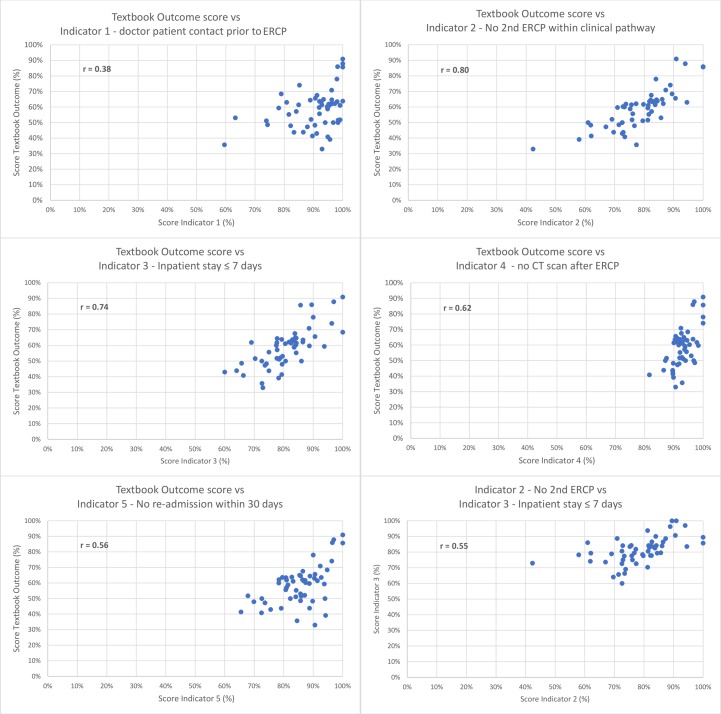
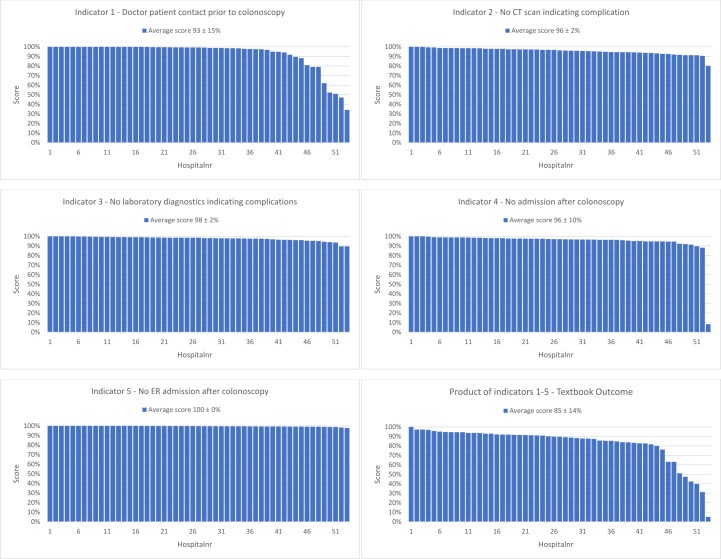
Results: Patients undergoing endoscopic retrograde cholangiopancreatography (ERCP) for gallstone disease (n=4369), colonoscopy for inflammatory bowel disease (IBD; n=19 330) and colonoscopy for colorectal cancer screening (n=22 149) were submitted to five suitable clinical indicators per treatment. The percentage of all patients who met all five criteria was 54%±9% (SD) for ERCP treatment. For IBD this was 47%±7% of the patients, and for colon cancer screening this number was 85%±14%.
Conclusion: This study shows that reusing data obtained from hospital information systems combined with clinical indicator definitions can be used to express short-term outcomes using the concept of Textbook Outcome without any excess registration. This information can provide meaningful insight into the clinical care trajectory on the level of individual patient care. Furthermore, this concept can be applied to many clinical trajectories within gastroenterology and beyond for monitoring and improving the clinical pathway and outcome for patients.
Keywords: performance measures; process mapping; quality in healthcare; standards of care.
© Article author(s) (or their employer(s) unless otherwise stated in the text of the article) 2018. All rights reserved. No commercial use is permitted unless otherwise expressly granted.
Conflict of interest statement
Competing interests: RHB has currently and NS had previously a relevant connection to LOGEX (Amsterdam, The Netherlands) as employees. LOGEX offers healthcare analytics to medical specialists. MV, RdM, PJdJ, BH and VE have no relevant connection to LOGEX.
Figures

Similar articles
-
Focusing on desired outcomes of care after colon cancer resections; hospital variations in 'textbook outcome'.Eur J Surg Oncol. 2013 Feb;39(2):156-63. doi: 10.1016/j.ejso.2012.10.007. Epub 2012 Oct 25. Eur J Surg Oncol. 2013. PMID: 23102705
-
Evaluating the validity of quality indicators for colorectal cancer care.J Surg Oncol. 2013 Dec;108(7):465-71. doi: 10.1002/jso.23420. Epub 2013 Sep 20. J Surg Oncol. 2013. PMID: 24115008
-
Combining process indicators to evaluate quality of care for surgical patients with colorectal cancer: are scores consistent with short-term outcome?BMJ Qual Saf. 2012 Jun;21(6):481-9. doi: 10.1136/bmjqs-2011-000439. Epub 2012 Apr 4. BMJ Qual Saf. 2012. PMID: 22491528
-
Endoscopic biliopancreatic investigations and therapy.Best Pract Res Clin Gastroenterol. 2008;22(5):865-81. doi: 10.1016/j.bpg.2008.05.004. Best Pract Res Clin Gastroenterol. 2008. PMID: 18790436 Review.
-
Quality indicators for endoscopic retrograde cholangiopancreatography.Gastrointest Endosc. 2006 Apr;63(4 Suppl):S29-34. doi: 10.1016/j.gie.2006.02.019. Gastrointest Endosc. 2006. PMID: 16564909 Review. No abstract available.
Cited by
-
Analysis of textbook outcomes for ampullary carcinoma patients following pancreaticoduodenectomy.World J Gastrointest Surg. 2023 Oct 27;15(10):2259-2271. doi: 10.4240/wjgs.v15.i10.2259. World J Gastrointest Surg. 2023. PMID: 37969713 Free PMC article.
-
The value of analyzing textbook outcomes after laparoscopic hepatectomy-a narrative review.Transl Cancer Res. 2023 Mar 31;12(3):631-637. doi: 10.21037/tcr-22-2122. Epub 2023 Feb 22. Transl Cancer Res. 2023. PMID: 37033349 Free PMC article. Review.
-
Comparing textbook outcomes among patients undergoing surgery for cancer at U. S. News & World Report ranked hospitals.J Surg Oncol. 2020 May;121(6):927-935. doi: 10.1002/jso.25833. Epub 2020 Mar 2. J Surg Oncol. 2020. PMID: 32124433 Free PMC article.
-
Predictors of textbook outcome following oesophagogastric cancer surgery.Dis Esophagus. 2024 Jul 3;37(7):doae023. doi: 10.1093/dote/doae023. Dis Esophagus. 2024. PMID: 38525934 Free PMC article.
-
Achieving textbook outcome in liver resection for hepatocellular carcinoma: malnutrition's pivotal role.Langenbecks Arch Surg. 2025 Apr 23;410(1):139. doi: 10.1007/s00423-025-03703-x. Langenbecks Arch Surg. 2025. PMID: 40266358 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous