

Renal replacement therapy in Europe-a summary of the 2009 ERA-EDTA Registry Annual Report
- PMID: 29497512
- PMCID: PMC5783206
- DOI: 10.1093/ndtplus/sfr182
Renal replacement therapy in Europe-a summary of the 2009 ERA-EDTA Registry Annual Report
Abstract
Introduction: This study provides a summary of the 2009 ERA-EDTA Registry Report, with a focus on the differences in the incidence and prevalence of haemodialysis (HD), peritoneal dialysis (PD) and renal transplantation between countries and over time.
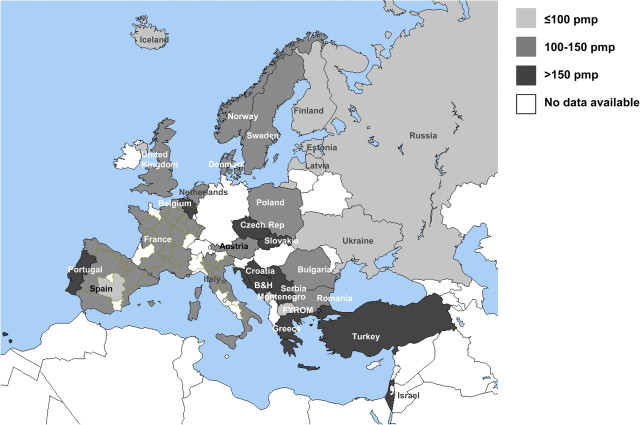
Methods: For this report, 56 data sets on renal replacement therapy (RRT) from national and regional registries in 30 countries in Europe and bordering the Mediterranean Sea were available. Data sets with individual patient data were received from 26 registries, whereas 19 registries contributed data in aggregated form. For both types of registries, we present incidence, prevalence and transplant rates. Survival analysis is based on individual patient records.
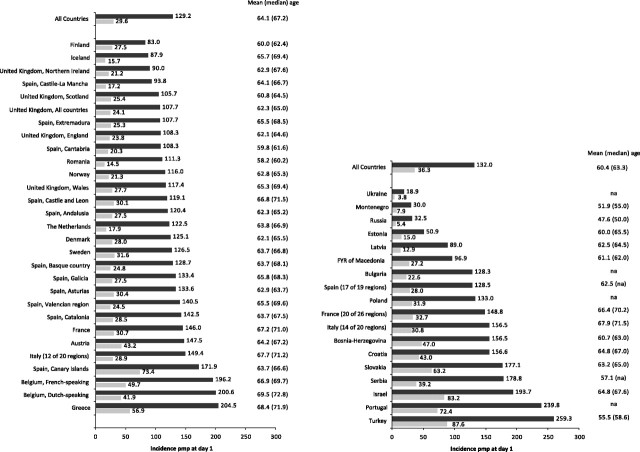
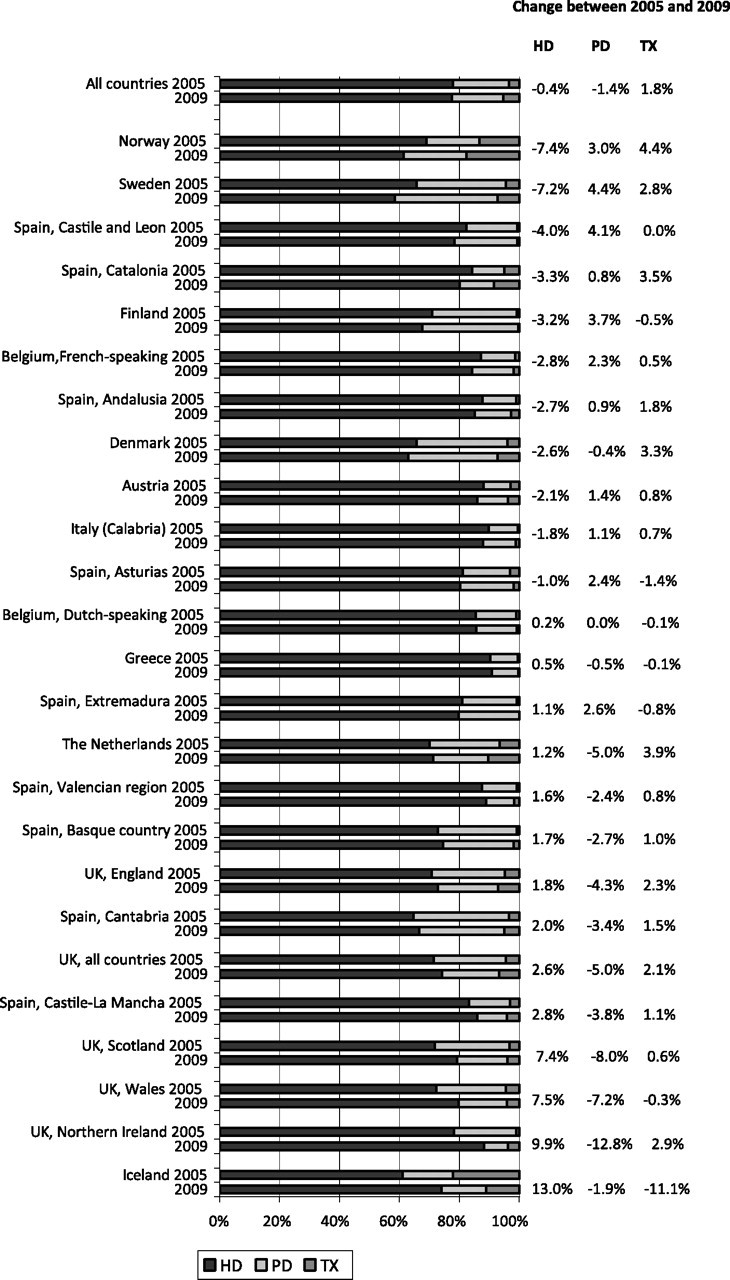
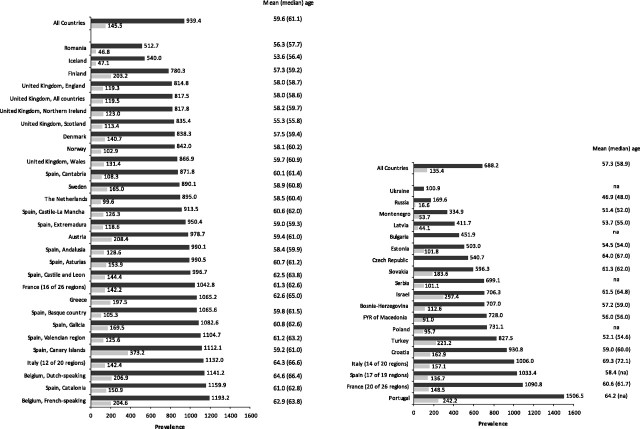
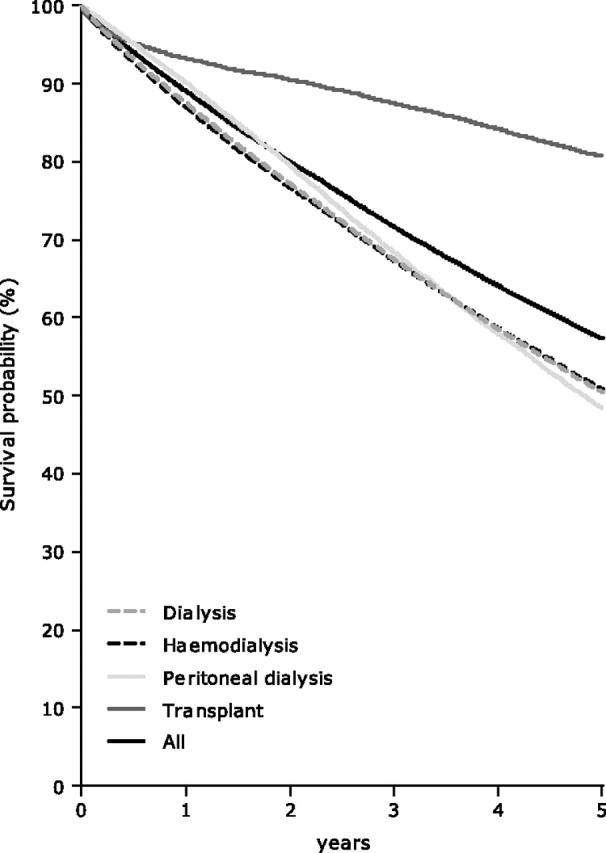
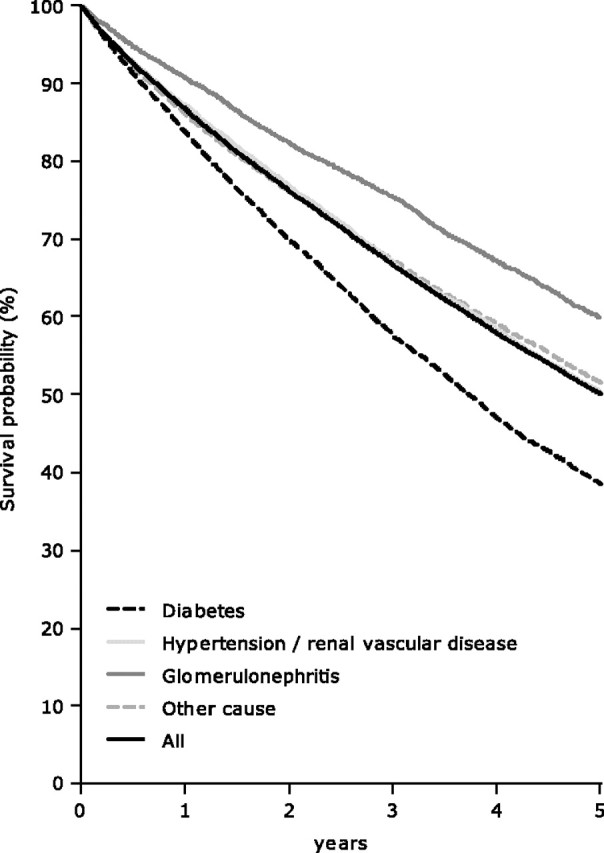
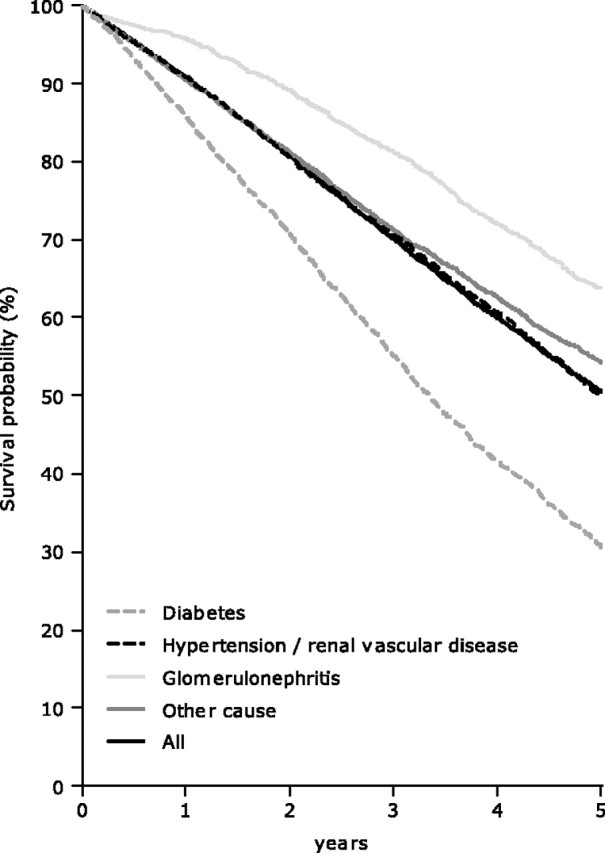
Results: In 2009, the overall incidence rate of RRT for end-stage renal disease (ESRD) among all registries reporting to the ERA-EDTA Registry was 125 per million population (p.m.p.). Incidence rates varied from 259 p.m.p. in Turkey to 19 p.m.p. in Ukraine and the mean age of patients starting RRT in 2009 ranged from 47.6 years in Russia to 69.5 year in Dutch-speaking Belgium. When examining the relative change of the HD, PD and transplantation distribution (at Day 91 after the start of RRT) between 2005 and 2009, we found overall a 0.5% decrease in HD, 1.4% decrease in PD utilization and an 1.8% increase of the share of patients living on a functioning graft. The overall prevalence of RRT for ESRD as of 31 December 2009 was 730 p.m.p. The highest prevalence was reported by Portugal (1507 p.m.p.) and the lowest by Ukraine (101 p.m.p.). In Norway, 70% of the patients on RRT were living with a functioning graft (591 p.m.p.) at 31 December 2009. The number of transplants performed p.m.p. in 2009 was highest in Spain (Cantabria) (78 p.m.p.). For the cohort 2000-04, the adjusted 1-, 2- and 5-year survival of patients on RRT was 87.4% (95% confidence interval: 87.2-87.7), 78.5% (95% confidence interval: 78.2-78.8) and 56.3% (95% confidence interval: 55.9-56.7), respectively.
Keywords: dialysis; incidence; prevalence; survival; transplantation.
Figures
References
-
- ERA-EDTA Registry. Amsterdam, The Netherlands: Academic Medical Center, Department of Medical Informatics; 2011. ERA-EDTA Registry Annual Report 2009.
LinkOut - more resources
Full Text Sources
