

Prospective observational study of 177Lu-DOTA-octreotate therapy in 200 patients with advanced metastasized neuroendocrine tumours (NETs): feasibility and impact of a dosimetry-guided study protocol on outcome and toxicity
- PMID: 29497803
- PMCID: PMC5915504
- DOI: 10.1007/s00259-018-3945-z
Prospective observational study of 177Lu-DOTA-octreotate therapy in 200 patients with advanced metastasized neuroendocrine tumours (NETs): feasibility and impact of a dosimetry-guided study protocol on outcome and toxicity
Abstract
Purpose: Peptide receptor radionuclide therapy in patients with neuroendocrine tumours has yielded promising results. This prospective study investigated the feasibility of dosimetry of the kidneys and bone marrow during therapy and its impact on efficacy and outcome.
Methods: The study group comprised 200 consecutive patients with metastasized somatostatin receptor-positive neuroendocrine tumours progressing on standard therapy or not suitable for other therapeutic options. A treatment cycle consisted of 7.4 GBq 177Lu-DOTA-octreotate with co-infusion of a mixed amino acid solution, and cycles were repeated until the absorbed dose to the kidneys reached 23 Gy or there were other reasons for stopping therapy. The Ki-67 index was ≤2% in 47 patients (23.5%), 3-20% in 121 (60.5%) and >20% in 16 (8%).
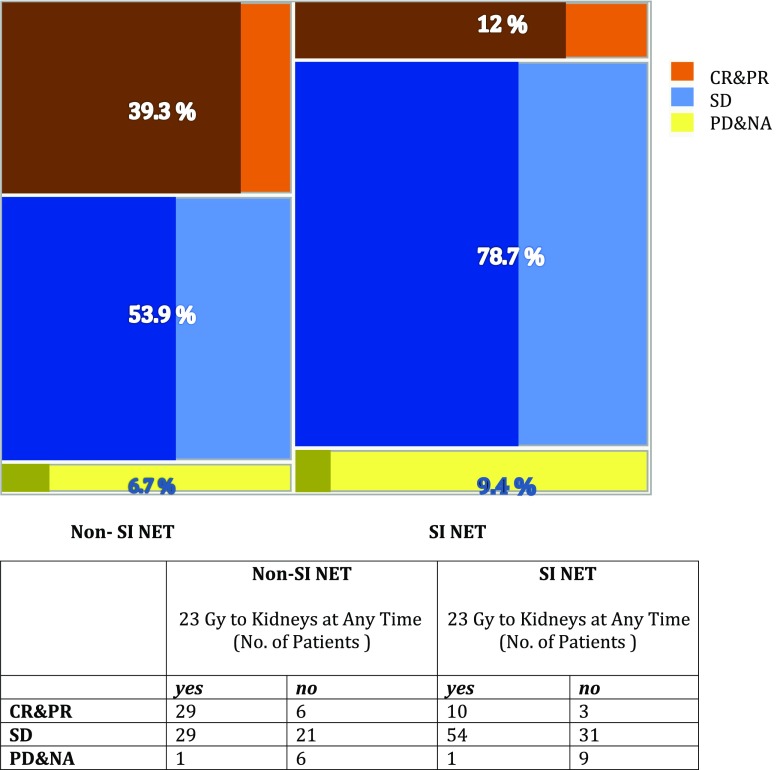
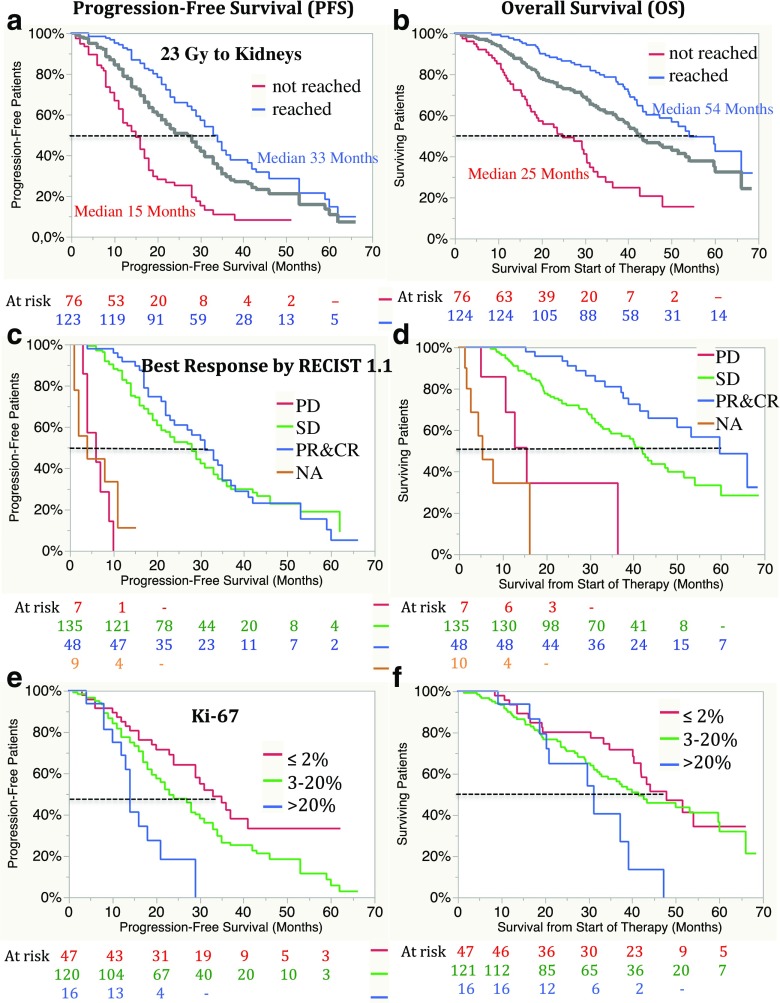
Results: In 123 patients (61.5%) the absorbed dose to the kidneys reached 23 Gy with three to nine cycles during first-line therapy; in no patient was a dose to the bone marrow of 2 Gy reached. The best responses (according to RECIST 1.1) were a complete response (CR) in 1 patient (0.5%), a partial response (PR) in 47 (23.5%), stable disease (SD) in 135 (67.5%) and progressive disease (PD) in 7 (3.5%). Median progression-free survival was 27 months (95% CI 22-30 months) in all patients, 33 months in those in whom the absorbed dose to the kidneys reached 23 Gy and 15 months in those in whom it did not. Median overall survival (OS) was 43 months (95% CI 39-53 months) in all patients, 54 months in those in whom the absorbed dose to the kidneys reached 23 Gy and 25 months in those in whom it did not. Median OS was 60 months in patients with a best response of PR or CR, 42 months in those with SD and 16 months in those with PD. Three patients (1.5%) developed acute leukaemia, 1 patient (0.5%) chronic leukaemia (unconfirmed) and 30 patients (15%) grade 3 or 4 bone marrow toxicity. Eight patients (4%) developed grade 2 kidney toxicity and one patient (0.5%) grade 4 kidney toxicity.
Conclusions: Dosimetry-based therapy with 177Lu-DOTA-octreotate is feasible. Patients in whom the absorbed dose to the kidneys reached 23 Gy had a longer OS than those in whom it did not. Patients with CR/PR had a longer OS than those with SD. Bone marrow dosimetry did not predict toxicity.
Keywords: 177Lu-DOTA-octreotate; Dosimetry; Neuroendocrine tumour; Outcome; PRRT; Toxicity.
Conflict of interest statement
Conflicts of interest
One of the authors (A.S.) is advisor to Advanced Accelerator Applications, France. All other authors declare no conflicts of interest.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the principles of the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Informed consent
Informed consent was obtained from all individual participants included in the study.
Figures




References
-
- Kwekkeboom DJ, Mueller-Brand J, Paganelli G, Anthony LB, Pauwels S, Kvols LK, et al. Overview of results of peptide receptor radionuclide therapy with 3 radiolabeled somatostatin analogs. J Nucl Med. 2005;46(Suppl 1):62S–66S. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
