

Hypertension after kidney donation: Incidence, predictors, and correlates
- PMID: 29498216
- PMCID: PMC6119643
- DOI: 10.1111/ajt.14713
Hypertension after kidney donation: Incidence, predictors, and correlates
Abstract
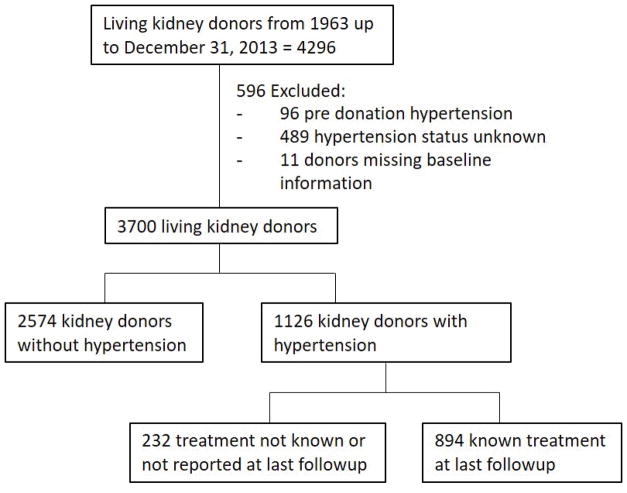
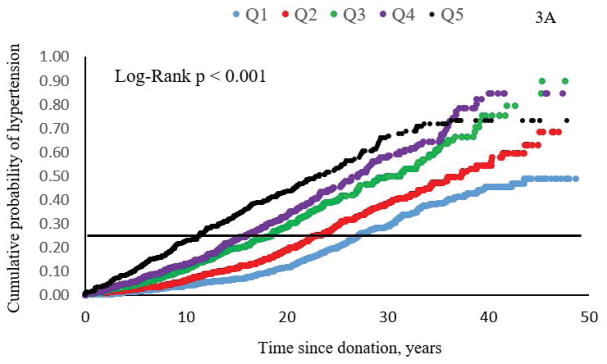
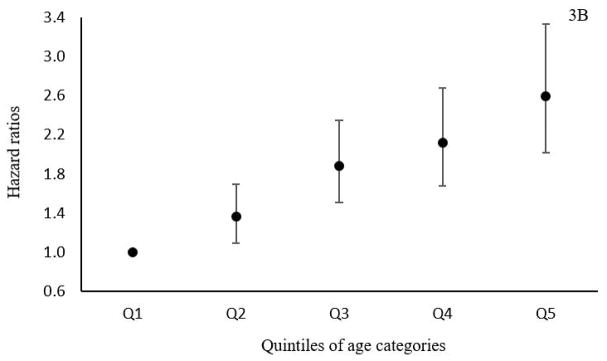
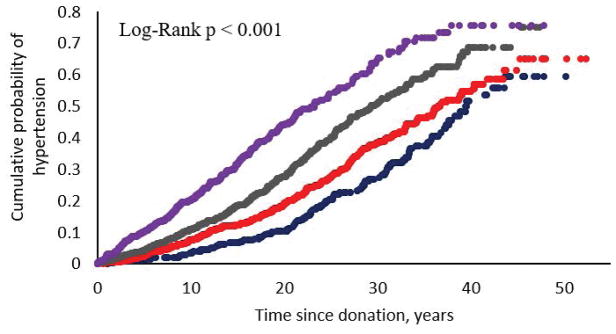
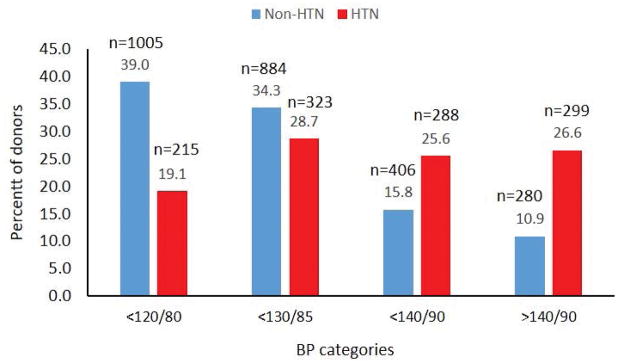
Incidence of postdonation hypertension, risk factors associated with its development, and impact of type of treatment received on renal outcomes were determined in 3700 kidney donors. Using Cox proportional hazard model, adjusted hazard ratios (HRs) for cardiovascular disease (CVD); estimated glomerular filtration rate (eGFR) <60, <45, <30 mL/min/1.73m2 ; end stage renal disease (ESRD); and death in hypertensive donors were determined. After a mean (standard deviation [SD]) of 16.6 (11.9) years of follow-up, 1126 (26.8%) donors developed hypertension and 894 with known antihypertensive medications. Hypertension developed in 4%, 10%, and 51% at 5, 10, and 40 years, respectively, and was associated with proteinuria, eGFR < 30, 45, and 60 mL/min/1.73m2 , CVD, and death. Blood pressure was <140/90 mm Hg at last follow-up in 75% of hypertensive donors. Use of angiotensin-converting enzyme inhibitors or angiotensin receptor blockers (compared to other antihypertensive agents) was associated with a lower risk for eGFR <45 mL/min/1.73m², HR 0.64 (95% confidence interval [CI] 0.45-0.9), P = .01, and also less ESRD; HR 0.03 (95% CI 0.001-0.20), P = .004. In this predominantly Caucasian cohort, hypertension is common after donation, well controlled in most donors, and factors associated with its development are similar to those in the general population.
Keywords: clinical research/practice; donors and donation: donor follow-up; epidemiology; hypertension/antihypertensives; kidney transplantation/nephrology.
© 2018 The American Society of Transplantation and the American Society of Transplant Surgeons.
Figures

References
-
- Brenner BM, Garcia DL, Anderson S. Glomeruli and blood pressure. Less of one, more the other? Am J Hypertens. 1988;1(4 Pt 1):335–347. - PubMed
-
- Kanzaki G, Tsuboi N, Haruhara K, Koike K, Ogura M, Shimizu A, et al. Factors associated with a vicious cycle involving a low nephron number, hypertension and chronic kidney disease. Hypertens Res. 2015;38(10):633–641. - PubMed
-
- Kasiske BL, Ma JZ, Louis TA, Swan SK. Long-term effects of reduced renal mass in humans. Kidney Int. 1995;48(3):814–819. - PubMed
-
- Boudville N, Prasad GV, Knoll G, Muirhead N, Thiessen-Philbrook H, Yang RC, et al. Meta-analysis: risk for hypertension in living kidney donors. Ann Intern Med. 2006;145(3):185–196. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
