

Chronic kidney disease and poor outcomes in ischemic stroke: is impaired cerebral autoregulation the missing link?
- PMID: 29499637
- PMCID: PMC5834853
- DOI: 10.1186/s12883-018-1025-4
Chronic kidney disease and poor outcomes in ischemic stroke: is impaired cerebral autoregulation the missing link?
Abstract
Background: Chronic kidney disease increases stroke incidence and severity but the mechanisms behind this cerebro-renal interaction are mostly unexplored. Since both vascular beds share similar features, microvascular dysfunction could be the possible missing link. Therefore, we examined the relationship between renal function and cerebral autoregulation in the early hours post ischemia and its impact on outcome.
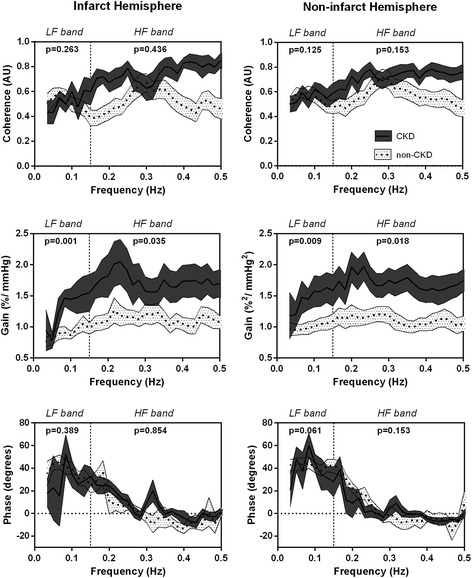
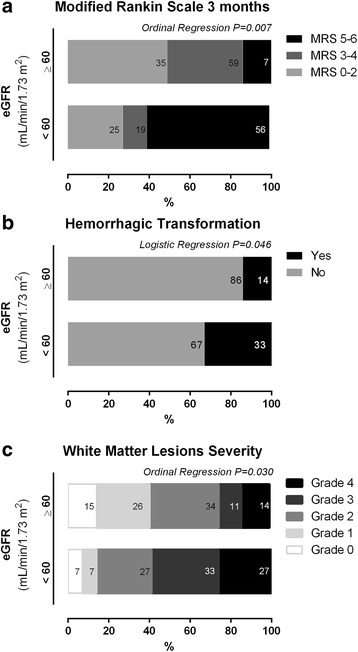
Methods: We enrolled 46 ischemic strokes (middle cerebral artery). Dynamic cerebral autoregulation was assessed by transfer function (coherence, phase and gain) of spontaneous blood pressure oscillations to blood flow velocity within 6 h from symptom-onset. Estimated glomerular filtration rate (eGFR) was calculated. Hemorrhagic transformation (HT) and white matter lesions (WML) were collected from computed tomography performed at presentation and 24 h. Outcome was evaluated with modified Rankin Scale at 3 months.
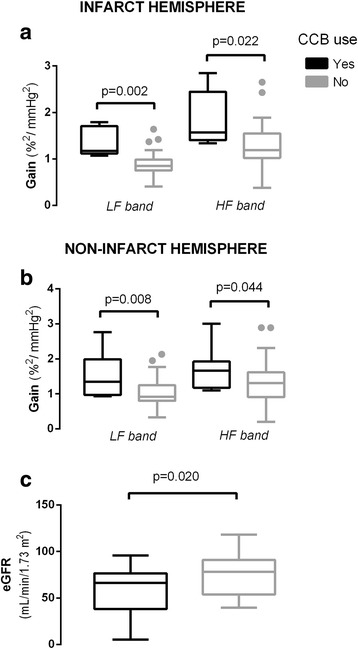
Results: High gain (less effective autoregulation) was correlated with lower eGFR irrespective of infarct side (p < 0.05). Both lower eGFR and higher gain correlated with WML grade (p < 0.05). Lower eGFR and increased gain, alone and in combination, progressively reduced the odds of a good functional outcome [ipsilateral OR = 4.39 (CI95% 3.15-25.6), p = 0.019; contralateral OR = 8.15 (CI95% 4.15-15.6), p = 0.002] and increased risk of HT [ipsilateral OR = 3.48 (CI95% 0.60-24.0), p = 0.132; contralateral OR = 6.43 (CI95% 1.40-32.1), p = 0.034].
Conclusions: Lower renal function correlates with less effective dynamic cerebral autoregulation in acute ischemic stroke, both predicting a bad outcome. The evaluation of serum biomarkers of renal dysfunction could have interest in the future for assessing cerebral microvascular risk and relationship with stroke complications.
Keywords: Cardiovascular disease; Chronic kidney disease; Glomerular filtration rate; Stroke; transcranial Doppler.
Conflict of interest statement
Ethics approval and consent to participate
The study was conducted in Hospital Center São João, Porto, and its local ethical committee approved the study and all participants or proxy signed written informed consent.
Consent for publication
Not applicable
Competing interests
Jorge Serrador is a member of the editorial board (Associate Editor) of this journal.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures


References
-
- Weiner DE, Tighiouart H, Amin MG, Stark PC, MacLeod B, Griffith JL, Salem DN, Levey AS, Sarnak MJ. Chronic kidney disease as a risk factor for cardiovascular disease and all-cause mortality: a pooled analysis of community-based studies. J Am Soc Nephrol. 2004;15(5):1307–1315. doi: 10.1097/01.ASN.0000123691.46138.E2. - DOI - PubMed
-
- Naganuma M, Koga M, Shiokawa Y, Nakagawara J, Furui E, Kimura K, Yamagami H, Okada Y, Hasegawa Y, Kario K, et al. Reduced estimated glomerular filtration rate is associated with stroke outcome after intravenous rt-PA: the stroke acute management with urgent risk-factor assessment and improvement (SAMURAI) rt-PA registry. Cerebrovasc Dis. 2011;31(2):123–129. doi: 10.1159/000321516. - DOI - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
