

Primaquine-induced haemolysis in females heterozygous for G6PD deficiency
- PMID: 29499733
- PMCID: PMC5833093
- DOI: 10.1186/s12936-018-2248-y
Primaquine-induced haemolysis in females heterozygous for G6PD deficiency
Abstract
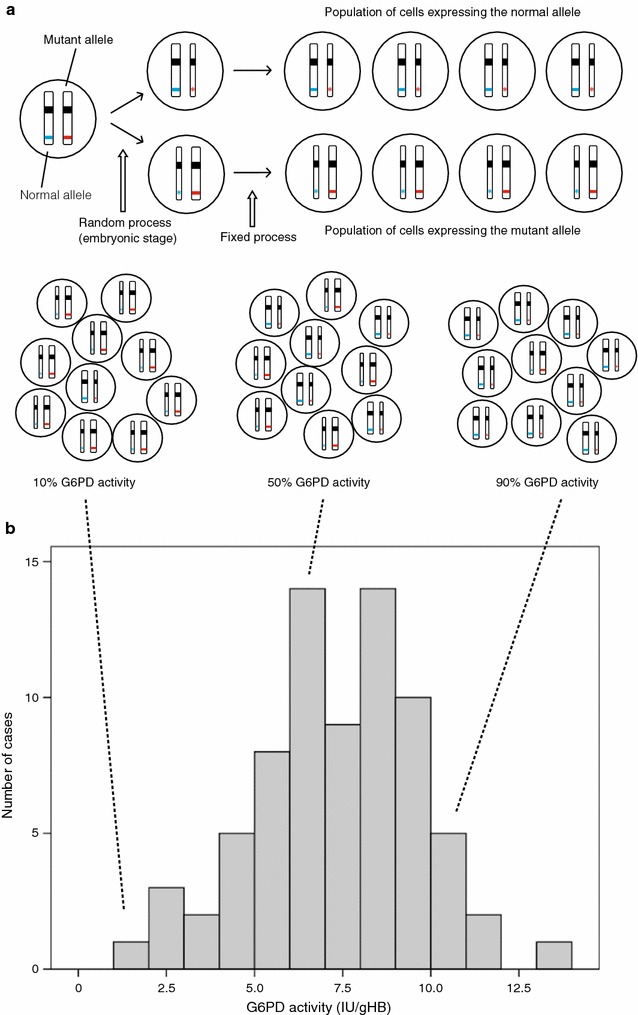
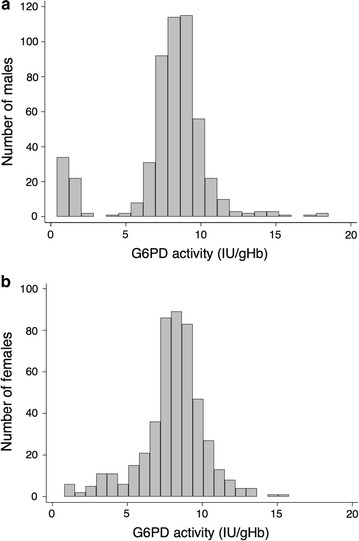
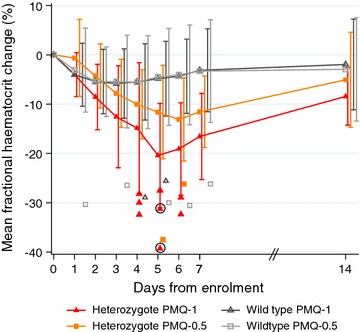
Oxidative agents can cause acute haemolytic anaemia in persons with G6PD deficiency. Understanding the relationship between G6PD genotype and the phenotypic expression of the enzyme deficiency is necessary so that severe haemolysis can be avoided. The patterns of oxidative haemolysis have been well described in G6PD deficient hemizygous males and homozygous females; and haemolysis in the proportionally more numerous heterozygous females has been documented mainly following consumption of fava beans and more recently dapsone. It has long been known that 8-aminoquinolines, notably primaquine and tafenoquine, cause acute haemolysis in G6PD deficiency. To support wider use of primaquine in Plasmodium vivax elimination, more data are needed on the haemolytic consequences of 8-aminoquinolines in G6PD heterozygous females. Two recent studies (in 2017) have provided precisely such data; and the need has emerged for the development of point of care quantitative testing of G6PD activity. Another priority is exploring alternative 8-aminoquinoline dosing regimens that are practical and improve safety in G6PD deficient individuals.
Keywords: 8-aminoquinoline; G6PD deficiency; G6PD heterozygous female; Haemolysis; Malaria; Plasmodium vivax; Primaquine; Radical cure.
Figures
References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
