

Efficacy of self-monitored blood pressure, with or without telemonitoring, for titration of antihypertensive medication (TASMINH4): an unmasked randomised controlled trial
- PMID: 29499873
- PMCID: PMC5854463
- DOI: 10.1016/S0140-6736(18)30309-X
Efficacy of self-monitored blood pressure, with or without telemonitoring, for titration of antihypertensive medication (TASMINH4): an unmasked randomised controlled trial
Abstract
Background: Studies evaluating titration of antihypertensive medication using self-monitoring give contradictory findings and the precise place of telemonitoring over self-monitoring alone is unclear. The TASMINH4 trial aimed to assess the efficacy of self-monitored blood pressure, with or without telemonitoring, for antihypertensive titration in primary care, compared with usual care.
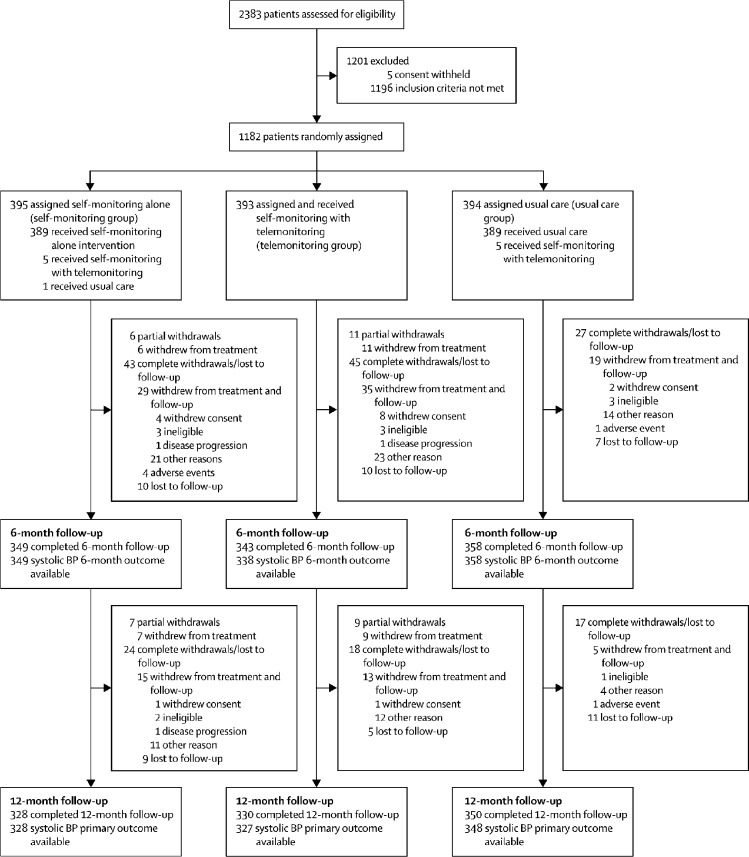
Methods: This study was a parallel randomised controlled trial done in 142 general practices in the UK, and included hypertensive patients older than 35 years, with blood pressure higher than 140/90 mm Hg, who were willing to self-monitor their blood pressure. Patients were randomly assigned (1:1:1) to self-monitoring blood pressure (self-montoring group), to self-monitoring blood pressure with telemonitoring (telemonitoring group), or to usual care (clinic blood pressure; usual care group). Randomisation was by a secure web-based system. Neither participants nor investigators were masked to group assignment. The primary outcome was clinic measured systolic blood pressure at 12 months from randomisation. Primary analysis was of available cases. The trial is registered with ISRCTN, number ISRCTN 83571366.
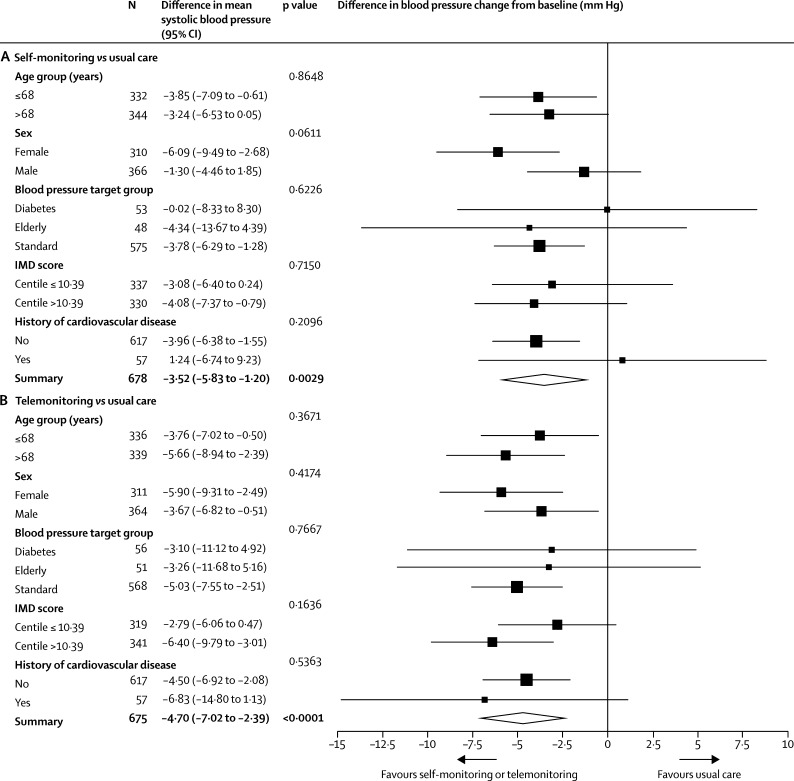
Findings: 1182 participants were randomly assigned to the self-monitoring group (n=395), the telemonitoring group (n=393), or the usual care group (n=394), of whom 1003 (85%) were included in the primary analysis. After 12 months, systolic blood pressure was lower in both intervention groups compared with usual care (self-monitoring, 137·0 [SD 16·7] mm Hg and telemonitoring, 136·0 [16·1] mm Hg vs usual care, 140·4 [16·5]; adjusted mean differences vs usual care: self-monitoring alone, -3·5 mm Hg [95% CI -5·8 to -1·2]; telemonitoring, -4·7 mm Hg [-7·0 to -2·4]). No difference between the self-monitoring and telemonitoring groups was recorded (adjusted mean difference -1·2 mm Hg [95% CI -3·5 to 1·2]). Results were similar in sensitivity analyses including multiple imputation. Adverse events were similar between all three groups.
Interpretation: Self-monitoring, with or without telemonitoring, when used by general practitioners to titrate antihypertensive medication in individuals with poorly controlled blood pressure, leads to significantly lower blood pressure than titration guided by clinic readings. With most general practitioners and many patients using self-monitoring, it could become the cornerstone of hypertension management in primary care.
Funding: National Institute for Health Research via Programme Grant for Applied Health Research (RP-PG-1209-10051), Professorship to RJM (NIHR-RP-R2-12-015), Oxford Collaboration for Leadership in Applied Health Research and Care, and Omron Healthcare UK.
Copyright © 2018 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Hypertension: time for doctors to switch the driver's seat?Lancet. 2018 Mar 10;391(10124):914-916. doi: 10.1016/S0140-6736(18)30317-9. Epub 2018 Feb 27. Lancet. 2018. PMID: 29499874 No abstract available.
-
Blutdruck am besten selbst messen.MMW Fortschr Med. 2018 May;160(8):30. doi: 10.1007/s15006-018-0473-5. MMW Fortschr Med. 2018. PMID: 29721882 Review. German. No abstract available.
-
There's no place like home: is self-monitoring beneficial in hypertension management?Kidney Int. 2018 Sep;94(3):450-452. doi: 10.1016/j.kint.2018.06.021. Kidney Int. 2018. PMID: 30143063 No abstract available.
-
Self-monitoring of blood pressure to guide titration of antihypertensive medication-a new era in hypertension management?Cardiovasc Diagn Ther. 2019 Feb;9(1):94-99. doi: 10.21037/cdt.2018.08.01. Cardiovasc Diagn Ther. 2019. PMID: 30881886 Free PMC article. No abstract available.
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
