

Cardiovascular and renal burdens of prediabetes in the USA: analysis of data from serial cross-sectional surveys, 1988-2014
- PMID: 29500121
- PMCID: PMC6615033
- DOI: 10.1016/S2213-8587(18)30027-5
Cardiovascular and renal burdens of prediabetes in the USA: analysis of data from serial cross-sectional surveys, 1988-2014
Abstract
Background: There is controversy over the usefulness of prediabetes as a diagnostic label. Using data from US National Health and Nutrition Examination Surveys (NHANES) between 1988 and 2014, we examined the cardiovascular and renal burdens in adults with prediabetes over time and compared patterns with other glycaemic status groups.
Methods: We analysed cross-sectional survey data from non-pregnant adults aged 20 years and older from the NHANES survey periods 1988-94, 1999-2004, 2005-10, and 2011-14. We defined diagnosed diabetes as patients' self-report that they had been previously diagnosed by a physician or health professional; among those with no self-reported diabetes, prediabetes was defined as a fasting plasma glucose (FPG) concentration of 100-125 mg/dL (5·6-6·9 mmol/L) or an HbA1c of 5·7-6·4% (39-47 mmol/mol); undiagnosed diabetes as an FPG of 126 mg/dL (7·0 mmol/L) or higher or an HbA1c of 6·5% (48 mmol/mol) or higher; and normal glycaemic status as an FPG of less than 100 mg/dL (5·6 mmol/L) and an HbA1c of less than 5·7% (39 mmol/mol). We repeated the analyses using varying definitions of prediabetes (FPG 110-125 mg/dL [6·1-6·9 mmol/L] or HbA1c 5·7-6·4% [39-47 mmol/mol], FPG 110-125 mg/dL [6·1-6·9 mmol/L] or HbA1c 6·0-6·4% [42-47 mmol/mol], and FPG 100-125 mg/dL [5·6-6·9 mmol/L] and HbA1c 5·7-6·4% [39-47 mmol/mol]). For each group over time, we estimated the prevalences of hypertension and dyslipidaemia; and among individuals with those conditions, we estimated the proportions who had been treated and who were achieving care goals. By glycaemic group, we estimated those who were current, former, and never smokers; mean 10-year risk of cardiovascular disease (using estimators from the Framingham Heart Study, the United Kingdom Prospective Diabetes Study (UKPDS), and the ACC/AHA ASCVD guidelines); albuminuria (median and albumin-to-creatinine ratio ≥30 mg/g), estimated glomerular filtration rate (eGFR; mean and <60 mL/min per 1·73m2); and prevalence of myocardial infarction and stroke. For all estimates, we calculated predicted changes between 1988-94 and 2011-14 using logistic regression models adjusted for age, sex, and race or ethnic group.
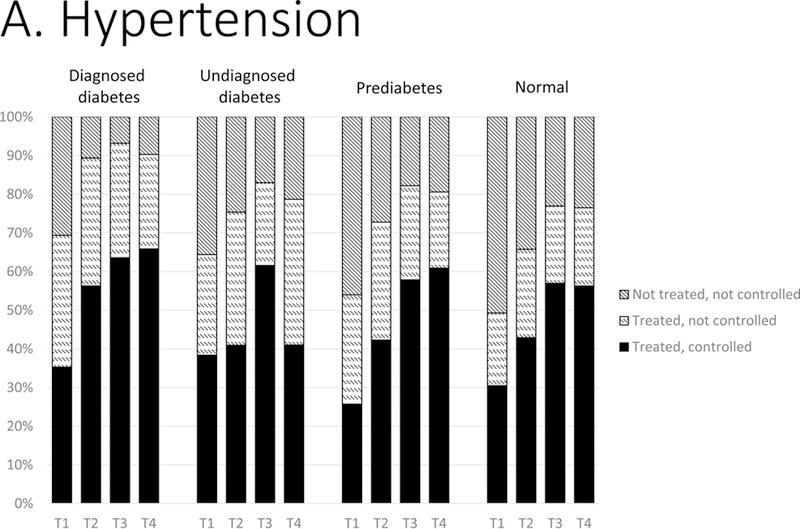
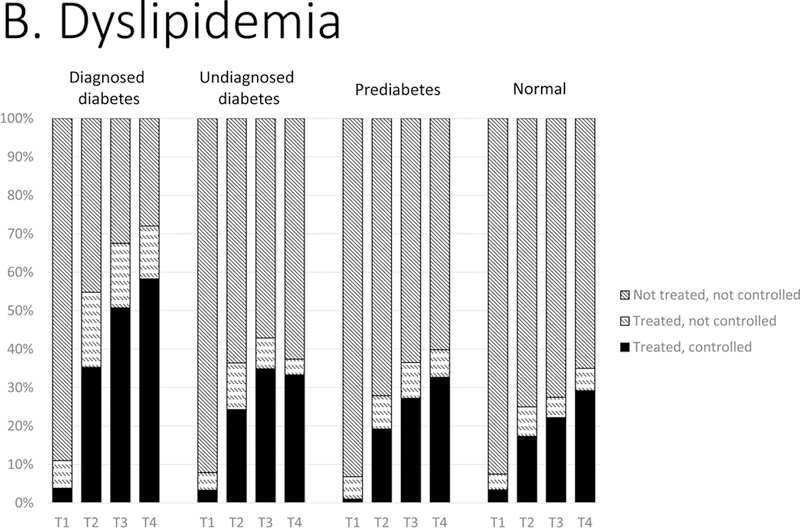
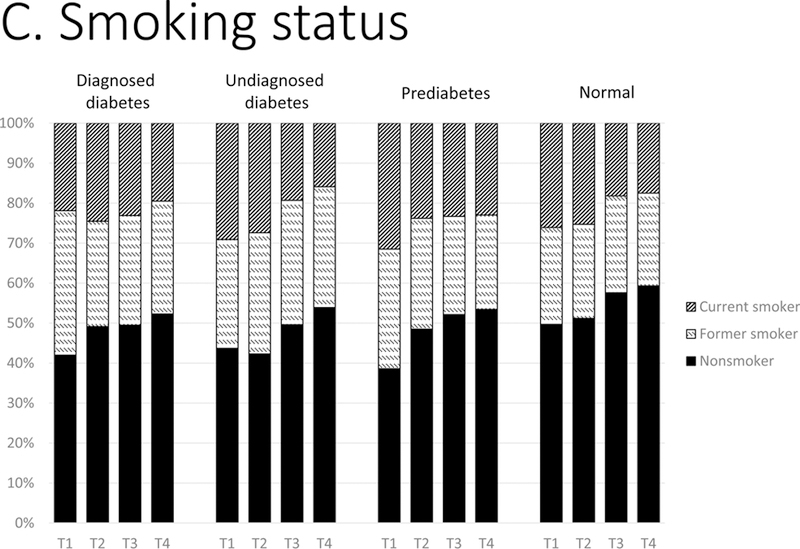
Findings: We obtained data for 27 971 eligible individuals. In 2011-14, in the population of adults with prediabetes, 36·6% (95% CI 32·8-40·5) had hypertension, 51·2% (47·0-55·3) had dyslipidaemia, 24·3% (21·7-27·3) smoked; 7·7% (6·8-8·8) had albuminuria; 4·6% (3·7-5·9) had reduced eGFR; and 10-year cardiovascular event risk ranged from 5% to 7%. From 1988-94 to 2011-14, adults with prediabetes showed significant increases in hypertension (+9·7 percentage points [95% CI 5·4-14·0]); no change in dyslipidaemia; decreases in smoking (-6·4 percentage points [-10·7 to -2·1]); increased use of treatment to lower blood pressure (54·2% [49·0-59·3] to 81·4% [76·7-85·3], +27·2 percentage points [20·5-33·8] p<0·0001) and to reduce lipids (6·6% to 40·2%, +33·6 percentage points [30·2-37·0], p<0·0001); and increased goal achievements for blood pressure (25·8% to 62·0%, +36·2 percentage points [30·7-41·8], p<0·0001) and lipids (1·0% to 32·8%, +31·8 percentage points [29·1-34·4, p<0·0001]). People with prediabetes also showed decreases in cardiovascular risk (ASCVD -1·9 percentage points [-2·5 to -1·3] to UKPDS -2·7 [-3·5 to -1·9], p<0·0001); but no change in prevalence of albuminuria, reduced eGFR, myocardial infarction, or stroke. Prevalence and patterns were consistent across all prediabetes definitions examined. Compared with adults with prediabetes, adults with diagnosed diabetes showed much larger improvements in cardiovascular and renal risk treatments, apart from smoking, which did not decline.
Interpretation: Over 25 years, cardiovascular and renal risks and disease have become highly prevalent in adults with prediabetes, irrespective of the definitions used. Identification of people with prediabetes might increase the opportunity for cardiovascular and renal risk reduction.
Funding: None.
Copyright © 2018 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Does addressing prediabetes help to improve population health?Lancet Diabetes Endocrinol. 2018 May;6(5):354-356. doi: 10.1016/S2213-8587(18)30030-5. Epub 2018 Feb 27. Lancet Diabetes Endocrinol. 2018. PMID: 29500120 No abstract available.
References
-
- Gerstein HC, Santaguida P, Raina P, Morrison KM, Balion C, Hunt D, et al. Annual incidence and relative risk of diabetes in people with various categories of dysglycemia: a systematic overview and meta-analysis of prospective studies. Diabetes Res Clin Pract. 2007;78(3):305–12. - PubMed
-
- Morris DH, Khunti K, Achana F, Srinivasan B, Gray LJ, Davies MJ, et al. Progression rates from HbAlc 6.0–6.4% and other prediabetes definitions to type 2 diabetes: a meta-analysis. Diabetologia. 2013;56(7):1489–93. - PubMed
-
- Tuomilehto J, Lindstrom J, Eriksson JG, Valle TT, Hamalainen H, Ilanne-Parikka P, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344(18):1343–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
