

[3D augmented reality visualization for navigated osteosynthesis of pelvic fractures]
- PMID: 29500506
- PMCID: PMC5898194
- DOI: 10.1007/s00113-018-0466-y
[3D augmented reality visualization for navigated osteosynthesis of pelvic fractures]
Abstract
Background: Despite great advances in the development of hardware and software components, surgical navigation systems have only seen limited use in current clinical settings due to their reported complexity, difficulty of integration into clinical workflows and questionable advantages over traditional imaging modalities.
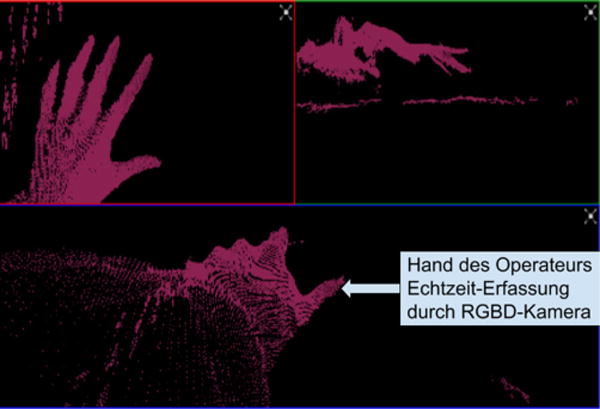
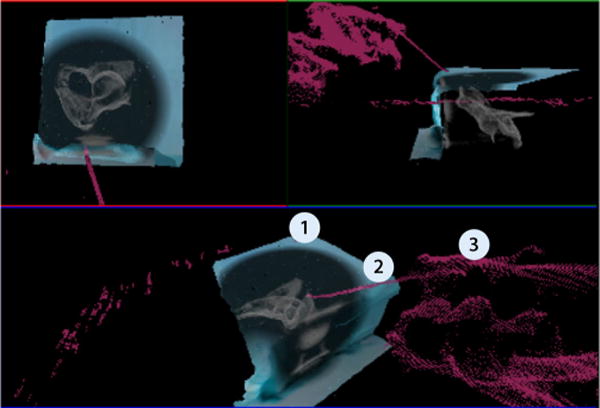
Objectives: Development of augmented reality (AR) visualization for surgical navigation without the need for infrared (IR) tracking markers and comparison of the navigation system to conventional imaging.
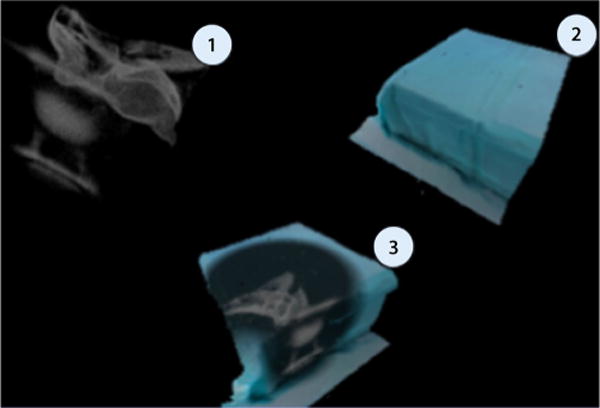
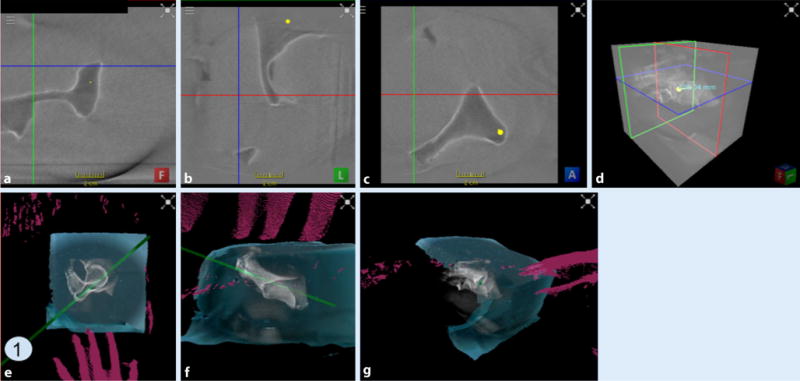
Material and methods: Novel navigation system combining a cone beam computed tomography (CBCT) capable C‑arm with a red-green-blue depth (RGBD) camera. Testing of the device by Kirschner wire (K-wire) placement in phantoms and evaluation of the necessary operating time, number of fluoroscopic images and overall radiation dose were compared to conventional x‑ray imaging.
Results: We found a significant reduction of the required time, number of fluoroscopic images and overall radiation dose in 3D AR navigation in comparison to x‑ray imaging.
Conclusion: Our AR navigation using RGBD cameras offers a flexible and intuitive visualization of the operating field for the navigated osteosynthesis without IR tracking markers, enabling surgeons to complete operations quicker and with a lower radiation exposure to the patient and surgical staff.
Hintergrund: Trotz großer Fortschritte in der Entwicklung der Hard- und Software von Navigationssystemen finden diese aufgrund ihrer vermeintlichen Komplexität, umständlichen Integration in klinische Arbeitsabläufe und fraglichen Vorteilen gegenüber konventionellen bildgebenden Verfahren bisher wenig Einsatz in den heutigen Operationssälen.
Ziel der Arbeit: Entwicklung einer „Augmented-reality“(AR)-Darstellung zur chirurgischen Navigation ohne Infrarot(„IR“)-Tracking-Marker und Vergleich zum konventioneller Röntgen in einem simulierten Eingriff.
Material und Methoden: Navigationssystem bestehend aus „Cone-beam-CT“(CBCT)-fähigem C-Bogen und „Red-green-blue-depth“(RGBD)-Kamera. Testung durch Kirschner(K)-Draht-Platzierung in Modellen unter Berücksichtigung der benötigten Zeit, der Strahlendosis und der Benutzerfreundlichkeit der Systeme.
Ergebnisse: Eine signifikante Reduktion der benötigten Zeit, der Röntgenbilder und der gesamten Strahlendosis bei der AR-Navigation gegenüber dem konventionellen Röntgen bei gleichbleibender Präzision.
Schlussfolgerung: Die AR-Navigation mithilfe der RGBD-Kamera bietet flexible und intuitive Darstellungsmöglichkeiten des Operations-situs für navigierte Osteosynthesen ohne Tracking-Marker. Hiermit ist es möglich, Operationen schneller, einfacher und mit geringerer Strahlenbelastung für Patient und OP-Personal durchzuführen.
Keywords: Computer assisted surgery; Feasibility studies; Kirschner wires; Radiation exposure; Time factors.
Conflict of interest statement
Figures
References
-
- Routt MC, Jr, Simonian PT, Mills WJ. Iliosacral screw fixation: early complications of the percutaneous technique. J Orthop Trauma. 1997;11(8):584–589. - PubMed
-
- Guy P, Al-Otaibi M, Harvey EJ, Helmy N. The „safe zone“ for extraarticular screw placement during intrapelvic acetabular surgery. J Orthop Trauma. 2010;24(5):279–283. - PubMed
-
- Stöckle U, Schaser K, König B. Image guidance in pelvic and acetabular surgery expectations, success and limitations. Injury. 2007;38(4):450–462. - PubMed
-
- Matthews F, Hoigne DJ, Weiser M, Wanner GA, Regazzoni P, Suhm N, Messmer P. Navigating the fluoroscope’s C-arm back into position: an accurate and practicable solution to cut radiation and optimize intraoperative workflow. J Orthop Trauma. 2007;21(10):687–692. - PubMed
-
- Gebhard FT, Kraus MD, Schneider E, Liener UC, Kinzl L, Arand M. Does computerassisted spine surgery reduce intraoperative radiation doses? Spine. 2027;31(17):2024–2006. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
