

Levodopa improves response inhibition and enhances striatal activation in early-stage Parkinson's disease
- PMID: 29501966
- PMCID: PMC6436810
- DOI: 10.1016/j.neurobiolaging.2018.02.003
Levodopa improves response inhibition and enhances striatal activation in early-stage Parkinson's disease
Abstract
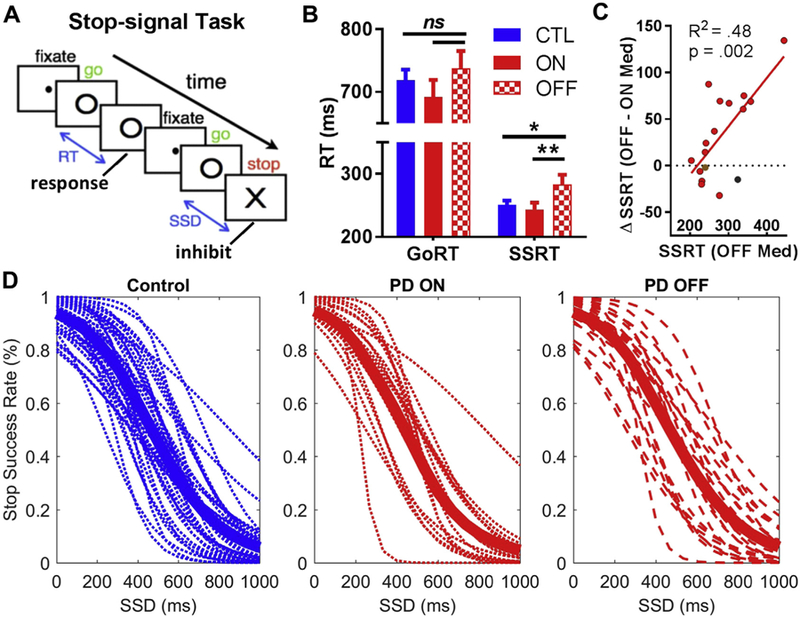
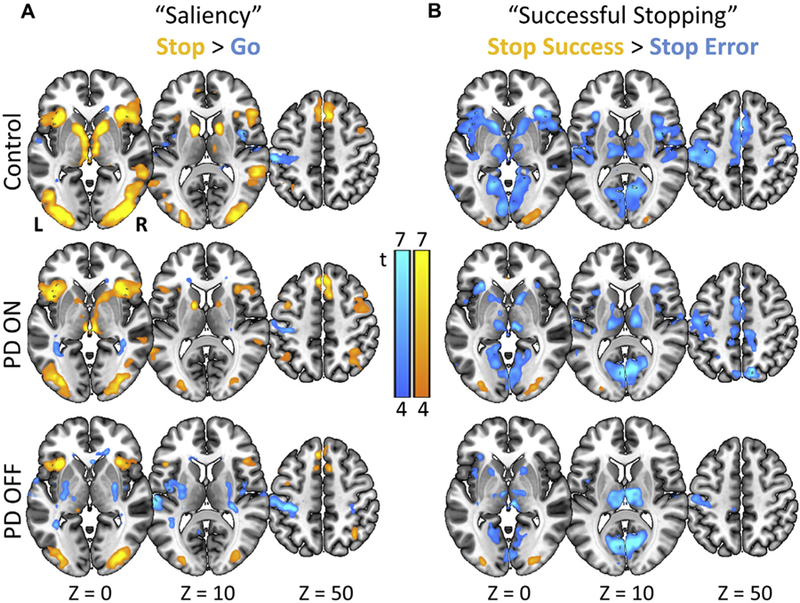
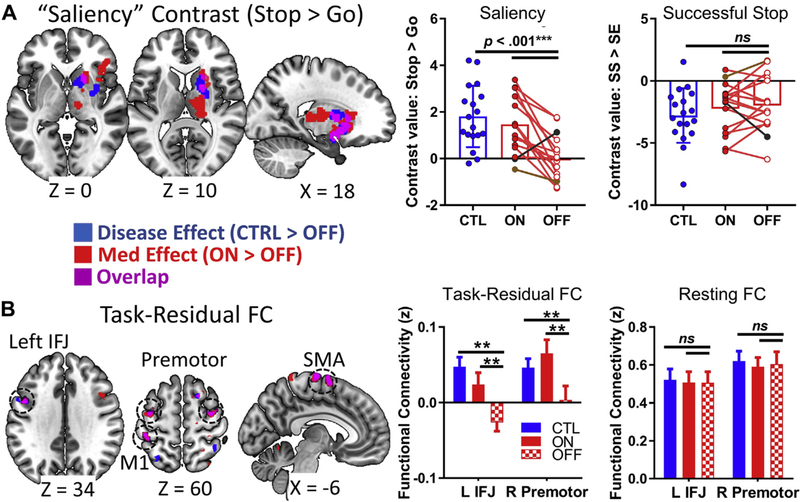
Dopaminergic medications improve the motor symptoms of Parkinson's disease (PD), but their effect on response inhibition, a critical executive function, remains unclear. Previous studies primarily enrolled patients in more advanced stages of PD, when dopaminergic medication loses efficacy, and patients were typically on multiple medications. Here, we recruited 21 patients in early-stage PD on levodopa monotherapy and 37 age-matched controls to perform the stop-signal task during functional magnetic resonance imaging. In contrast to previous studies reporting null effects in more advanced PD, levodopa significantly improved response inhibition performance in our sample. No significant group differences were found in brain activations to pure motor inhibition or error processing (stop success vs. error trials). However, relative to controls, the PD group showed weaker striatal activations to salient events (infrequent vs. frequent events: stop vs. go trials) and fronto-striatal task-residual functional connectivity; both were restored with levodopa. Thus, levodopa appears to improve an important executive function in early-stage PD via enhanced salient signal processing, shedding new light on the role of dopaminergic signaling in response inhibition.
Keywords: Basal ganglia; Cognitive control; Dopamine; Executive function; Movement disorders; Stop-signal task.
Published by Elsevier Inc.
Conflict of interest statement
Disclosure statement
The authors thank the Stony Brook Research Foundation for providing funds for participant stipend payment. The study is also supported by grant BCS1309260 (C-sRL) from the National Science Foundation. The authors have no competing interests to disclose.
Figures
References
-
- Alegre M, Lopez-Azcarate J, Obeso I, Wilkinson L, Rodriguez-Oroz MC, Valencia M, Garcia-Garcia D, Guridi J, Artieda J, Jahanshahi M, Obeso JA, 2013. The subthalamic nucleus is involved in successful inhibition in the stop-signal task: a local field potential study in Parkinson’s disease. Exp. Neurol 239, 1–12. - PubMed
-
- Andersson JLR, Skare S, Ashburner J, 2003. How to correct susceptibility distortions in spin-echo echo-planar images: application to diffusion tensor imaging. NeuroImage 20, 870–888. - PubMed
-
- Band GPH, van der Molen MW, Logan GD, 2003. Horse-race model simulations of the stop-signal procedure. Acta Psychologica 112, 105–142. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
