

Multiple primary non-breast tumors in breast cancer survivors
- PMID: 29502170
- PMCID: PMC11813444
- DOI: 10.1007/s00432-018-2621-9
Multiple primary non-breast tumors in breast cancer survivors
Abstract
Purpose: The aim of this study was to assess the frequency of second primary non-breast cancer after breast cancer diagnosis and treatment, and its correlation with clinicopathological features.
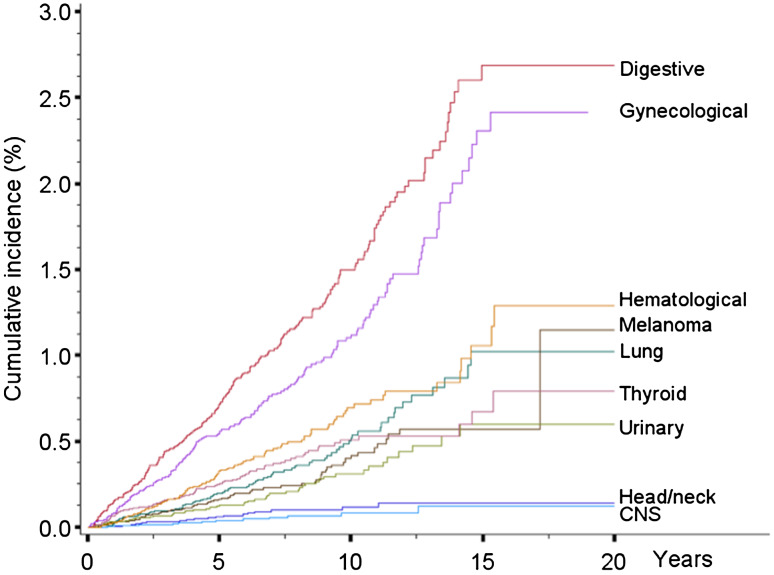
Methods: Data from 21,527 patients with primary breast cancer were collected retrospectively in a single cancer centre; 4.1% of the women developed a second non-breast cancer. The most frequently observed second primary tumor affected the digestive tract (27.8%). The frequency of observed cancers was similar to that expected in the general population, excepting for an excess of melanoma [SIR 1.98 (1.52-2.53)], uterine cancers [SIR 1.44 (1.17-1.74)], ovarian cancers [SIR 1.67 (1.31-2.10)], thyroid tumors [SIR 1.54 (1.23-1.92)], and leukemia [SIR 1.57 (1.11-2.16)].
Results: Clinicopathological breast cancer stratification showed a general increased risk of developing a second cancer in older patients, excluding ovarian cancer. An increased risk of developing ovarian cancer after breast cancer diagnosis was observed, in particular, in triple-negative [HR 3.47 (1.91-6.29)], G3 tumors [HR 2.54 (1.10-5.83)] and in positive breast cancer family history [HR 2.19 (1.22-3.94)]. Breast cancer survivors in hormonal therapy treatment are at higher risk for developing a second thyroid cancer [HR 4.00 (1.46-10.9)]. Conversely, adjuvant chemotherapy offered a protective effect on thyroid cancer risk development [HR 0.46 (0.28-0.76)].
Conclusions: Older age represents the major risk of developing a second primary non-breast cancer, excluding ovarian cancer. Clinical surveillance is required to prevent ovarian and thyroid cancers, respectively, in patients with positive family history, triple negative, G3 breast cancer and during hormonal therapy treatment in postmenopausal status.
Keywords: Breast cancer; Diagnosis; Second primary cancer; Treatment; Tumor staging.
Conflict of interest statement
The authors declare that they have no conflict of interest.
Figures
References
-
- Bray F, Ferlay J, Laversanne M, Brewster DH, Gombe Mbalawa C, Kohler B, Piñeros M, Steliarova-Foucher E, Swaminathan R, Antoni S, Soerjomataram I, Forman D (2015) Cancer incidence in five continents: inclusion criteria, highlights from volume X and the global status of cancer registration. Int J Cancer 13:2060–2071 - DOI - PubMed
-
- Corso G, Figueiredo J, Biffi R, Trentin C, Bonanni B, Feroce I, Serrano D, Cassano E, Annibale B, Melo S, Seruca R, De Lorenzi F, Ferrara F, Piagnerelli R, Roviello F, Galimberti V (2014) E-cadherin germline mutation carriers: clinical management and genetic implications. Cancer Metastasis Rev 33:1081–1094 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
