

Effect of Radiation Treatment Volume Reduction on Lymphopenia in Patients Receiving Chemoradiotherapy for Glioblastoma
- PMID: 29502931
- PMCID: PMC8362501
- DOI: 10.1016/j.ijrobp.2018.01.069
Effect of Radiation Treatment Volume Reduction on Lymphopenia in Patients Receiving Chemoradiotherapy for Glioblastoma
Abstract
Purpose: To evaluate whether reduction in glioblastoma radiation treatment volume can reduce risk of acute severe lymphopenia (ASL).
Methods and materials: A total of 210 patients with supratentorial/nonmetastatic glioblastoma were treated with radiation therapy (RT) plus temozolomide from 2007 to 2016 and had laboratory data on total lymphocyte counts. Before 2015, 164 patients were treated with standard-field RT (SFRT), and limited-field RT (LFRT) was implemented thereafter for 46 patients to reduce treatment volume. Total lymphocyte counts were evaluated at baseline, during RT, and at approximately week 12 from initiating RT. Acute severe lymphopenia was defined as any total lymphocyte count < 500 cells/μL within 3 months (by week 12) of initiating RT. Multivariate analysis for overall survival (OS) was performed with Cox regression and with logistic regression for ASL. Propensity score matching was performed to adjust for variability between cohorts. Acute severe lymphopenia, progression-free survival (PFS), and OS were compared using the Kaplan-Meier method.
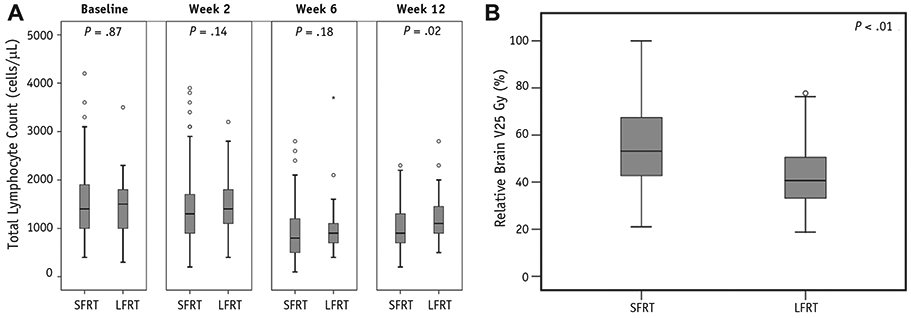
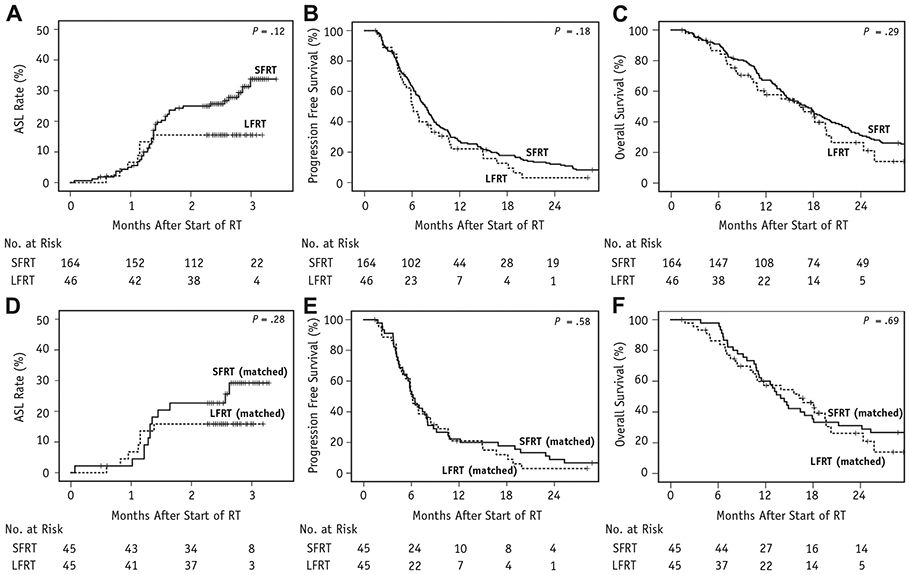
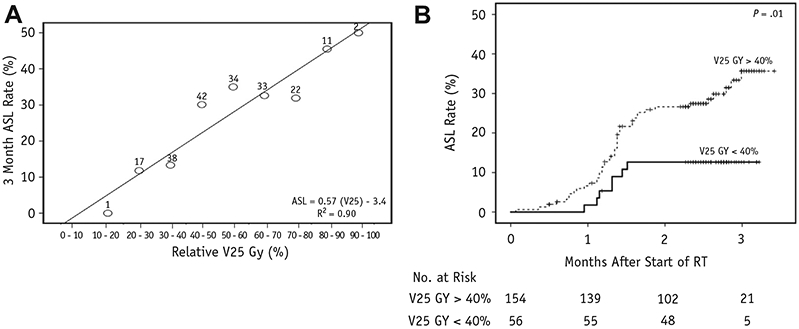
Results: Limited-field RT patients had higher gross tumor volume than SFRT patients yet lower brain dose-volume parameters, including volume receiving 25 Gy (V25 Gy: 41% vs 53%, respectively, P < .01). Total lymphocyte count at week 12 was significantly higher for LFRT than for SFRT (median: 1100 cells/μL vs 900 cells/μL, respectively, P = .02). On multivariate analysis, ASL was an independent predictor of OS, and brain V25 Gy was an independent predictor of ASL. The ASL rate at 3 months was 15.5% for LFRT and 33.8% for SFRT (P = .12). In a propensity-matched comparison of 45 pairs of LFRT and SFRT patients, PFS (median: 5.9 vs 6.2 months, respectively, P = .58) and OS (median: 16.2 vs 13.9 months, respectively, P = .69) were not significantly different.
Conclusions: Limited-field RT is associated with less lymphopenia after RT plus temozolomide and does not adversely affect PFS or OS. Brain V25 Gy is confirmed as an important dosimetric predictor for ASL.
Copyright © 2018 Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of interest: C.T. reports personal fees from Merck, personal fees from Varian, and personal fees from Novocure outside the submitted work.
Figures
References
-
- Stupp R, Taillibert S, Kanner AA, et al.Maintenance therapy with tumor-treating fields plus temozolomide vs temozolomide alone for glioblastoma: A randomized clinical trial. JAMA 2015;314:2535–2543. - PubMed
-
- Stupp R, Mason W, van den Bent MJ, et al.Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987–996. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
