

Treatment Strategy Based on Plaque Vulnerability and the Treatment Risk Evaluation for Internal Carotid Artery Stenosis
- PMID: 29503393
- PMCID: PMC5958040
- DOI: 10.2176/nmc.oa.2017-0228
Treatment Strategy Based on Plaque Vulnerability and the Treatment Risk Evaluation for Internal Carotid Artery Stenosis
Abstract
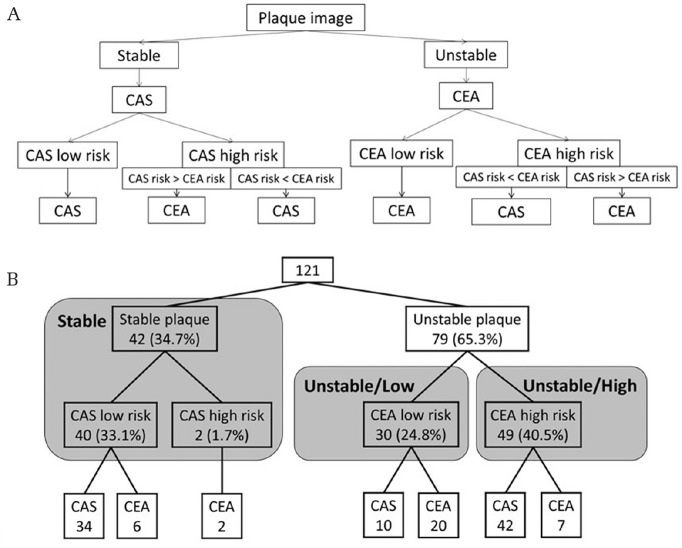
Carotid endarterectomy (CEA) and carotid artery stenting (CAS) are not appropriate treatment procedure for internal carotid artery stenosis (ICAS) in some patients. The importance of plaque vulnerability and the treatment risk evaluation has been reported. We analyzed whether treatment selection contributes to the outcome. We retrospectively examined 121 patients who underwent CEA or CAS. Treatment was selected based on plaque vulnerability and the treatment risk evaluation. We selected CAS for patients with stable plaques and CEA for patients with unstable plaques, and considered the other treatment for high-risk patients. The patients were classified as the stable plaque (Stable: n = 42), the unstable plaque and CEA low risk (Unstable/Low: n = 30), and the CEA high-risk (Unstable/High: n = 49). Frequency of perioperative stroke, myocardial infarction, death, and systemic complications was examined. CEA and CAS were performed in 35 and 86 patients, respectively. One patient (2.9%) had a stroke in CEA and five patients (5.8%) in CAS (P = 0.50). Systemic complications were observed in two patients (5.7%) in CEA and six (7.1%) in CAS (P = 0.80). There were no differences in stroke (Stable; 2.4%, Unstable/Low; 3.2%, and Unstable/High; 8.2%) and systemic complications (Stable; 9.5%, Unstable/Low; 3.3%, and Unstable/High; 6.1%) among three groups (P = 0.44 and P = 0.59, respectively). The treatment selection based on plaque vulnerability and the treatment risk evaluation could provide good treatment outcome for high-risk patients. It is ideal to select an appropriate treatment for ICAS by one neurovascular team.
Keywords: carotid artery stenting; carotid endarterectomy; internal carotid artery stenosis; plaque vulnerability; treatment risk evaluations.
Conflict of interest statement
YM received honoraria from Medtronic Japan and Stryker Japan for lecture fees. The other authors have no conflicts of interest. The authors registered online Self-reported COI Disclosure Statement Forms through the website for Japan Neurosurgical Society members.
Figures


References
-
- Mas JL, Chatellier G, Beyssen B, et al. EVA-3S Investigators : Endarterectomy versus stenting in patients with symptomatic severe carotid stenosis. N Engl J Med 355: 1660–1671, 2006 - PubMed
-
- Yadav JS, Wholey MH, Kuntz RE, et al. Stenting and Angioplasty with Protection in Patients at High Risk for Endarterectomy Investigators : Protected carotid-artery stenting versus endarterectomy in high-risk patients. N Engl J Med 351: 1493–1501, 2004 - PubMed
-
- SPACE Collaborative Group. Ringleb PA, Allenberg J, Brückmann H, et al. : 30 day results from the SPACE trial of stent-protected angioplasty versus carotid endarterectomy in symptomatic patients: a randomised non-inferiority trial. Lancet 368: 1239–1247, 2006 - PubMed
-
- International Carotid Stenting Study Investigators. Ederle J, Dobson J, Featherstone RL, et al. : Carotid artery stenting compared with endarterectomy in patients with symptomatic carotid stenosis (International Carotid Stenting Study): an interim analysis of a randomised controlled trial. Lancet 375: 985–997, 2010 - PMC - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources