

Role of palliative resection of the primary pancreatic neuroendocrine tumor in patients with unresectable metastatic liver disease: a systematic review and meta-analysis
- PMID: 29503572
- PMCID: PMC5827741
- DOI: 10.2147/OTT.S158171
Role of palliative resection of the primary pancreatic neuroendocrine tumor in patients with unresectable metastatic liver disease: a systematic review and meta-analysis
Abstract
Background: Treatment for pancreatic neuroendocrine tumors (PNETs) in patients with unresectable metastatic liver disease has long been a controversial issue. This systematic review aims to summarize the existing evidence concerning the value of primary tumor resection in this group of patients.
Methods: A systematic review of the literature and a meta-analysis were performed. The PubMed and Cochrane databases were searched to identify articles that compared palliative primary tumor resection and nonsurgical regimens in patients with PNETs and unresectable liver metastases. Relevant articles were identified in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. The primary outcome was overall survival. The included studies were evaluated for heterogeneity and publication bias.
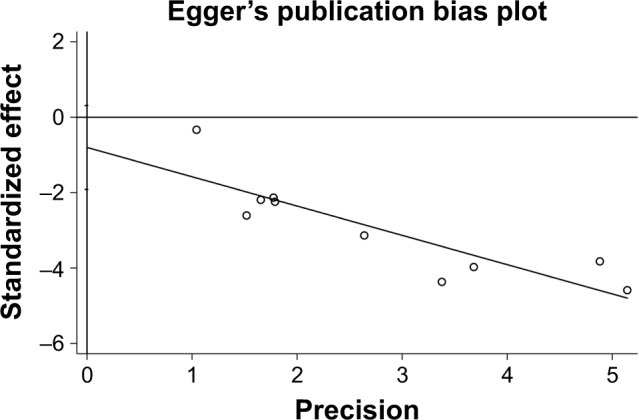
Results: Overall, 10 studies were included in the analysis. No randomized controlled trials (RCTs) were identified. These studies included 1,226 patients who underwent a resection of the primary tumor and 1,623 patients who did not undergo surgery. The median overall survival was 36-137 and 13.2-65 months in the surgical and nonsurgical groups, respectively, and the 5-year overall survival rate was 35.7-83 and 5.4%-50%, respectively, in these two groups. The meta-analysis demonstrated that there was no significant difference in liver tumor burden (odds ratio [OR] =1.51, 95% CI: 0.59-3.89, P=0.39) or tumor grade (OR =2.88, 95% CI: 0.92-9.04, P=0.07) among patients who underwent surgery and nonsurgical therapy. Furthermore, patients who underwent an aggressive surgical approach appeared to have a higher tumor grade. However, the meta-analysis demonstrated that patients who underwent primary tumor resection had better overall survival (P<0.001), with a pooled hazard ratio of 0.36 (95% CI: 0.30-0.45). No publication bias was detected.
Conclusion: This meta-analysis demonstrates that the palliative resection of the primary tumor in patients with PNETs and unresectable liver metastases can increase survival, although a bias toward a more aggressive surgical approach in patients with better performance status, less advanced disease, or a tumor located in the body or tail of the pancreas appears likely. RCTs with longer follow-up periods are required to confirm the advantages of palliative primary tumor resection for PNETs.
Keywords: liver metastases; pancreatic neuroendocrine tumors; prognosis; surgery.
Conflict of interest statement
Disclosure The authors report no conflicts of interest in this work.
Figures




References
-
- Modlin IM, Lye KD, Kidd M. A 5-decade analysis of 13,715 carcinoid tumors. Cancer. 2003;97(4):934–959. - PubMed
-
- Bilimoria KY, Talamonti MS, Tomlinson JS, et al. Prognostic score predicting survival after resection of pancreatic neuroendocrine tumors: analysis of 3851 patients. Ann Surg. 2008;247(3):490–500. - PubMed
-
- Chamberlain RS, Canes D, Brown KT, et al. Hepatic neuroendocrine metastases: does intervention alter outcomes? J Am Coll Surg. 2000;190(4):432–445. - PubMed
-
- Panzuto F, Nasoni S, Falconi M, et al. Prognostic factors and survival in endocrine tumor patients: comparison between gastrointestinal and pancreatic localization. Endocr Relat Cancer. 2005;12(4):1083–1092. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
