

Effect of Somatic Experiencing Resiliency-Based Trauma Treatment Training on Quality of Life and Psychological Health as Potential Markers of Resilience in Treating Professionals
- PMID: 29503607
- PMCID: PMC5820455
- DOI: 10.3389/fnins.2018.00070
Effect of Somatic Experiencing Resiliency-Based Trauma Treatment Training on Quality of Life and Psychological Health as Potential Markers of Resilience in Treating Professionals
Abstract
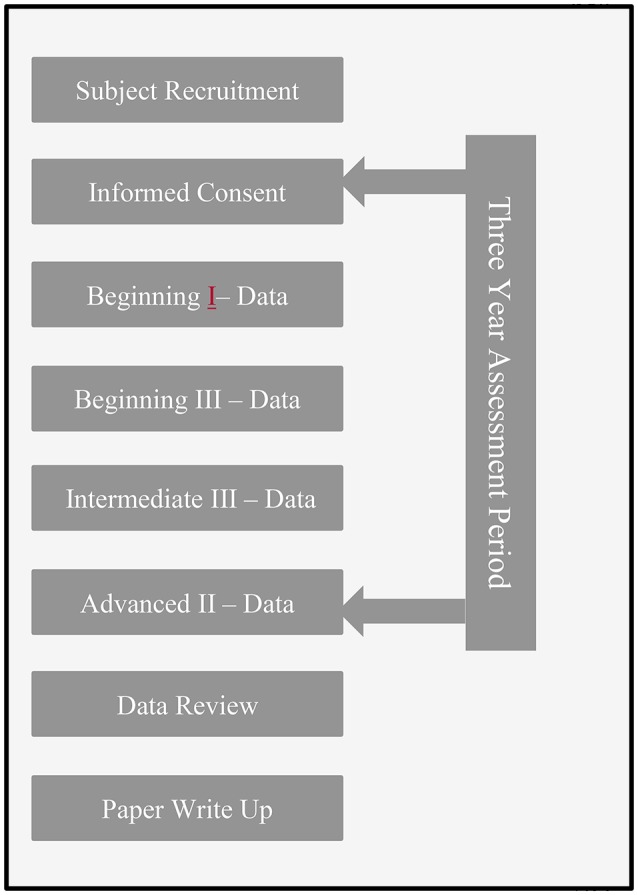
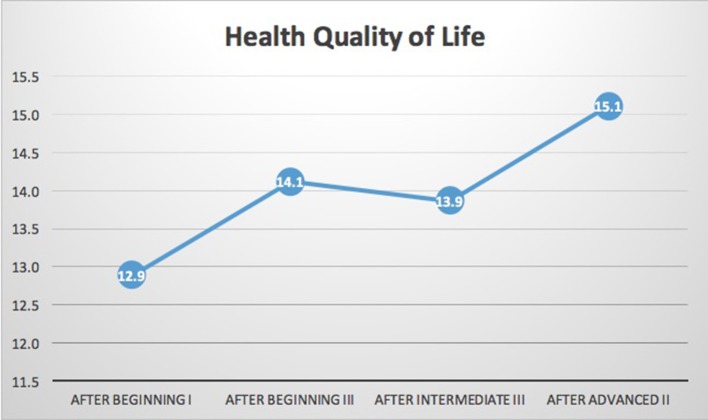
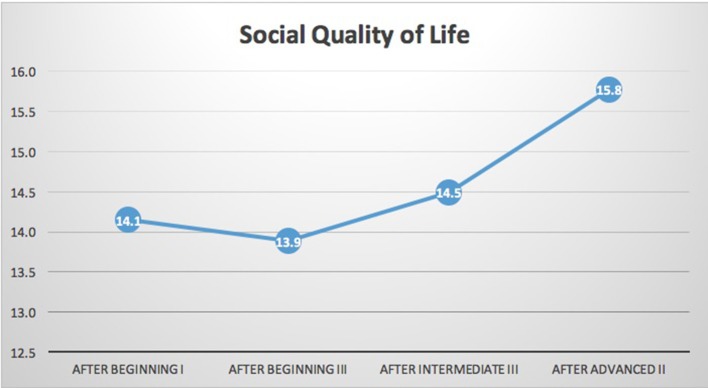
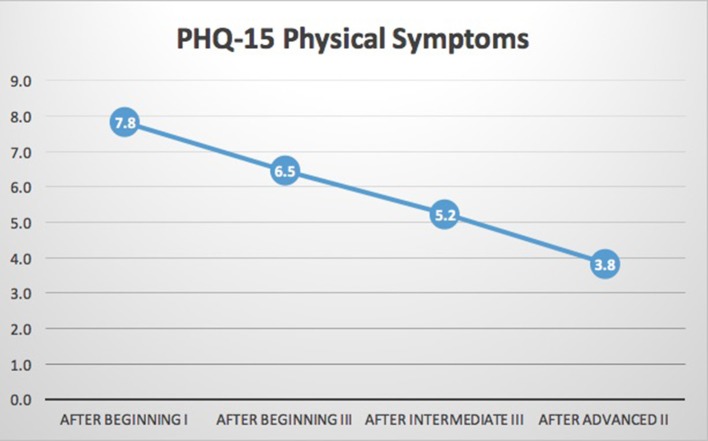
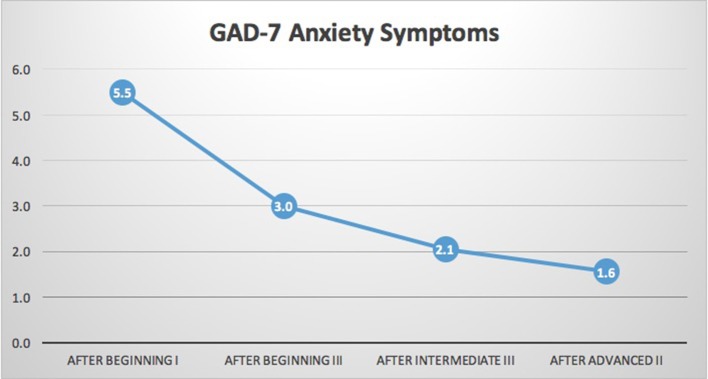
Background: Individuals who treat trauma are at significant risk of vicarious traumatization and burnout. Somatic Experiencing® (SE®) is a resiliency-focused trauma treatment modality designed to address autonomic nervous system (ANS) dysregulation and its impacted physical health and mental health symptoms e.g., anxiety, depression, post-traumatic stress disorder, migraines, fibromyalgia, and chronic fatigue, etc. The SE® training supports the development of clinical skills to reduce physical health/mental health symptoms as well as increase clinician resilience. Individuals who display resilience often have increased experiences of well-being (quality of life) and decreased levels of self-reported psychological symptoms. Greater resilience could mitigate the risks to providers and the clients they treat. Materials and Methods: This within-groups, longitudinal study assessed students (N = 18) over the course of a 3-year SE® practitioner training. This training focuses on increased ANS, physical, and emotional regulation skills. The convenience of a web-based survey allowed for: measures of a general quality of life (WHOQOL-BREF), psychological symptoms, somatic, anxiety, and depressive symptoms (PHQ-SADS), as well as a measure of early life exposure to adversity (CDC/Kaiser Permanente ACE Score Calculator Questionnaire). The clinician survey was conducted yearly for 3 years. Future studies would do well to also include laboratory-based objective measures of ANS functioning. Results: ANOVA with repeated measures showed that there were significant reductions in anxiety symptoms (GAD7, p < 0.001) and somatization symptoms (PHQ15, p < 0.001). Health-related quality of life (a measure of physical well-being) and social quality of life (a measure of interpersonal well-being) both increased significantly (Health QoL p = 0.028; Social QoL p = 0.046). Conclusions: Results suggest that professionals attending the 3-year SE® training course experience a significant improvement in self-reported measures associated with resiliency including: quality of life (well-being) and psychological symptoms (anxiety and somatization). Our results support the importance of future research in a larger sample and support the exploration, cross-sectionally and prospectively, of the relationship of clinician resiliency and changes in clinician resiliency with SE® training and clinical outcomes. These data have implications for other professions at risk of exposure to vicarious trauma (VT) including nurses, medical providers, and paramedics.
Keywords: ANS dysregulation; Somatic Experiencing®; burnout; compassion fatigue; quality of life; resiliency; traumatic stress; vicarious traumatization.
Figures
Similar articles
-
Somatic Experiencing® Informed Therapeutic Group for the Care and Treatment of Biopsychosocial Effects upon a Gender Diverse Identity.Front Psychiatry. 2018 Feb 27;9:53. doi: 10.3389/fpsyt.2018.00053. eCollection 2018. Front Psychiatry. 2018. PMID: 29535648 Free PMC article.
-
Military Health Provider Training and Evaluation of a Problem-Solving Intervention to Reduce Distress and Enhance Readiness Among Service Members.Mil Med. 2019 May 1;184(5-6):e303-e311. doi: 10.1093/milmed/usy229. Mil Med. 2019. PMID: 30252080
-
Quality of life across domains among individuals with treatment-resistant depression.J Affect Disord. 2019 Jan 15;243:401-407. doi: 10.1016/j.jad.2018.09.062. Epub 2018 Sep 19. J Affect Disord. 2019. PMID: 30268955 Free PMC article.
-
Does vicarious traumatisation affect oncology nurses? A literature review.Eur J Oncol Nurs. 2007 Sep;11(4):348-56. doi: 10.1016/j.ejon.2007.02.007. Epub 2007 May 7. Eur J Oncol Nurs. 2007. PMID: 17482879 Review.
-
Vicarious resilience: traversing the path from client to clinician through a search for meaning.Soc Work Health Care. 2022;61(6-8):468-482. doi: 10.1080/00981389.2022.2134274. Epub 2022 Oct 12. Soc Work Health Care. 2022. PMID: 36222370 Review.
Cited by
-
The Main Features of Resilience in Healthcare Providers: A Scoping Review.Med J Islam Repub Iran. 2022 Feb 3;36:3. doi: 10.47176/mjiri.36.3. eCollection 2022. Med J Islam Repub Iran. 2022. PMID: 35999934 Free PMC article.
-
Dealing with Emotional Vulnerability and Anxiety in Nurses from High-Risk Units-A Multicenter Study.Int J Environ Res Public Health. 2022 May 4;19(9):5569. doi: 10.3390/ijerph19095569. Int J Environ Res Public Health. 2022. PMID: 35564963 Free PMC article.
-
Do more stress and lower family economic status increase vulnerability to suicidal ideation? Evidence of a U-shaped relationship in a large cross-sectional sample of South Korean adolescents.PLoS One. 2021 Apr 26;16(4):e0250794. doi: 10.1371/journal.pone.0250794. eCollection 2021. PLoS One. 2021. PMID: 33901265 Free PMC article.
-
A Scoping Review of Vicarious Trauma Interventions for Service Providers Working With People Who Have Experienced Traumatic Events.Trauma Violence Abuse. 2022 Dec;23(5):1437-1460. doi: 10.1177/1524838021991310. Epub 2021 Mar 9. Trauma Violence Abuse. 2022. PMID: 33685294 Free PMC article.
-
A Network Model of Positive Resources, Temperament, Childhood Trauma, and Comorbid Symptoms for Patient with Depressive Disorders.Psychiatry Investig. 2021 Mar;18(3):214-224. doi: 10.30773/pi.2020.0187. Epub 2021 Mar 10. Psychiatry Investig. 2021. PMID: 33685037 Free PMC article.
References
-
- Bell H., Kulkarni S., Dalton L. (2003). Organizational prevention of vicarious trauma. Famil. Soc. J. Contemp. Soc. Ser. 84, 463–470. 10.1606/1044-3894.131 - DOI
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous