

Fatty Images of the Heart: Spectrum of Normal and Pathological Findings by Computed Tomography and Cardiac Magnetic Resonance Imaging
- PMID: 29503824
- PMCID: PMC5818975
- DOI: 10.1155/2018/5610347
Fatty Images of the Heart: Spectrum of Normal and Pathological Findings by Computed Tomography and Cardiac Magnetic Resonance Imaging
Abstract
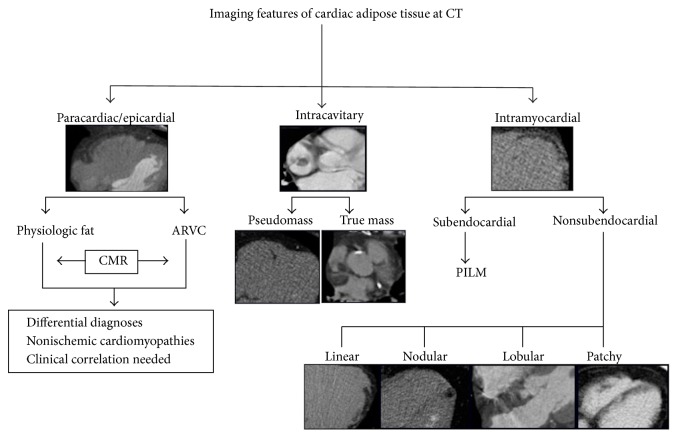
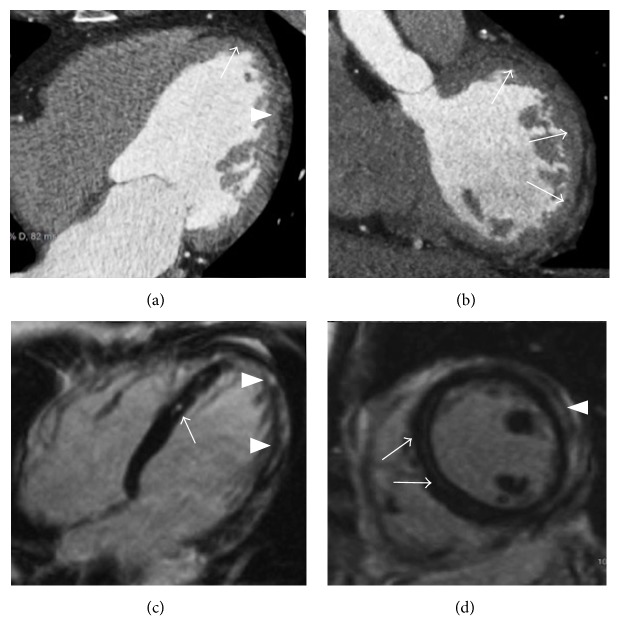
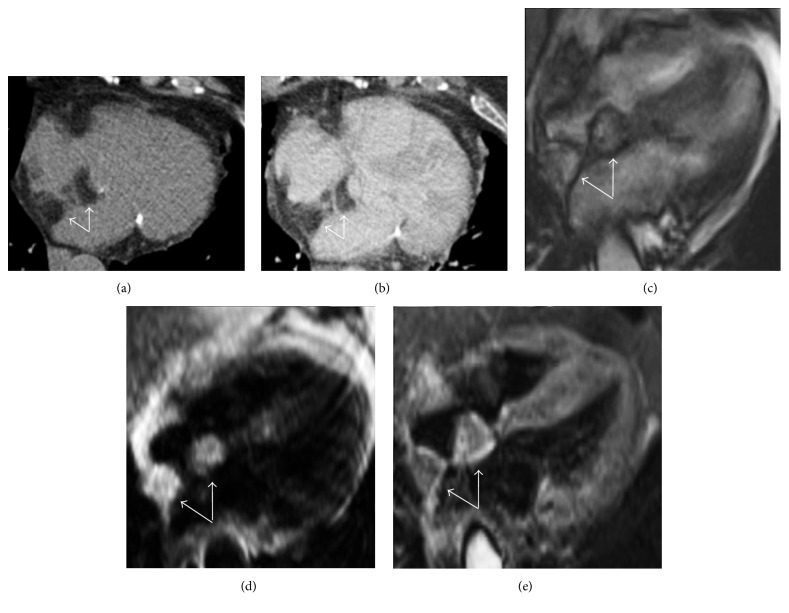
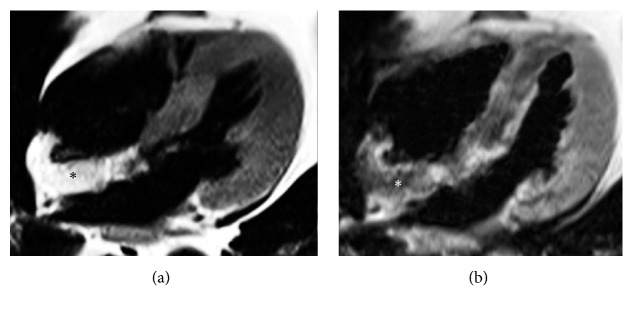
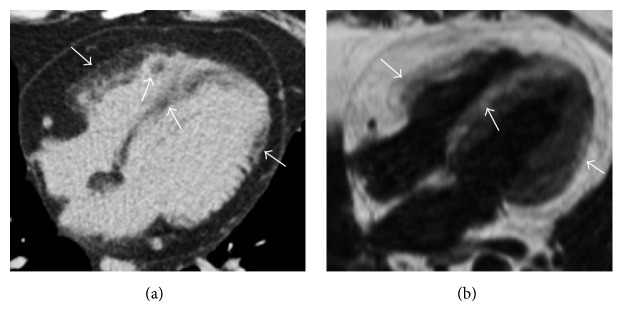
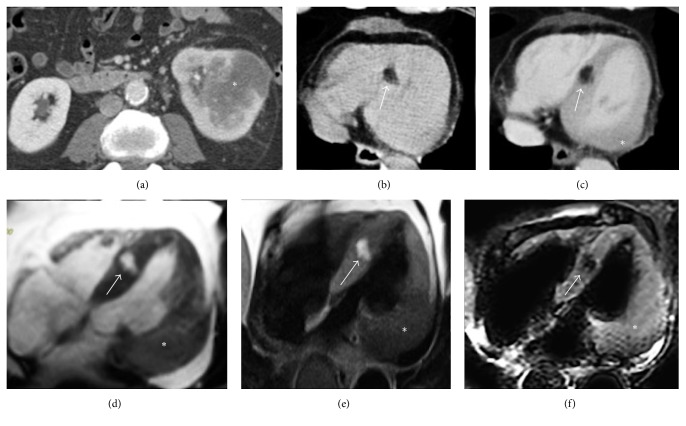
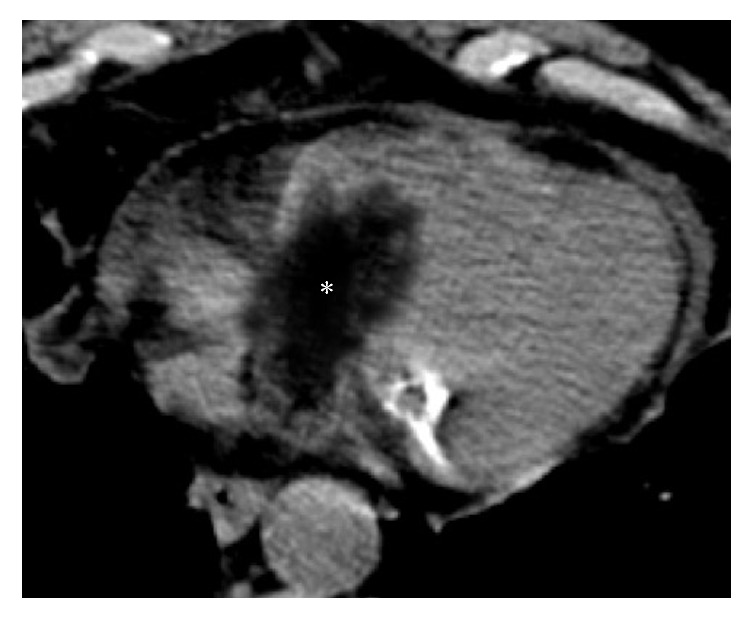
Ectopic cardiac fatty images are not rarely detected incidentally by computed tomography and cardiac magnetic resonance, or by exams focused on the heart as in general thoracic imaging evaluations. A correct interpretation of these findings is essential in order to recognize their normal or pathological meaning, focusing on the eventually associated clinical implications. The development of techniques such as computed tomography and cardiac magnetic resonance allowed a detailed detection and evaluation of adipose tissue within the heart. This pictorial review illustrates the most common characteristics of cardiac fatty images by computed tomography and cardiac magnetic resonance, in a spectrum of normal and pathological conditions ranging from physiological adipose images to diseases presenting with cardiac fatty foci. Physiologic intramyocardial adipose tissue may normally be present in healthy adults, being not related to cardiac affections and without any clinical consequence. However cardiac fatty images may also be the expression of various diseases, comprehending arrhythmogenic right ventricular dysplasia, postmyocardial infarction lipomatous metaplasia, dilated cardiomyopathy, and lipomatous hypertrophy of the interatrial septum. Fatty neoplasms of the heart as lipoma and liposarcoma are also described.
Figures
Similar articles
-
Myocardial fat at cardiac imaging: how can we differentiate pathologic from physiologic fatty infiltration?Radiographics. 2010 Oct;30(6):1587-602. doi: 10.1148/rg.306105519. Radiographics. 2010. PMID: 21071377
-
Fat-containing lesions of the chest.Radiographics. 2002 Oct;22 Spec No:S61-78. doi: 10.1148/radiographics.22.suppl_1.g02oc08s61. Radiographics. 2002. PMID: 12376601 Review.
-
Cardiac lipoma in a patient with proven arrhythmogenic right ventricular dysplasia: a case report. A huge intramyocardial lipoma.Int J Cardiovasc Imaging. 2005 Aug;21(4):463-7. doi: 10.1007/s10554-004-7024-0. Int J Cardiovasc Imaging. 2005. PMID: 16047131
-
Arrhythmogenic Right Ventricular Dysplasia: An Under-recognized Form of Inherited Cardiomyopathy.Rev Cardiovasc Med. 2017;18(1):37-43. doi: 10.3909/ricm0855. Rev Cardiovasc Med. 2017. PMID: 28509892 Review.
-
Images in cardiology. Visualising fatty deposits in familial arrhythmogenic right ventricular cardiomyopathy by magnetic resonance imaging.Heart. 2000 Jul;84(1):52. doi: 10.1136/heart.84.1.52. Heart. 2000. PMID: 10862588 Free PMC article. No abstract available.
Cited by
-
Longitudinal effect of myocardial fat deposition on left ventricular diastolic function: a retrospective cohort study.Int J Cardiovasc Imaging. 2022 May;38(5):955-961. doi: 10.1007/s10554-021-02483-x. Epub 2021 Nov 30. Int J Cardiovasc Imaging. 2022. PMID: 34846618
-
The Effect of Adiposity on Cardiovascular Function and Myocardial Fibrosis in Patients With Duchenne Muscular Dystrophy.J Am Heart Assoc. 2021 Oct 5;10(19):e021037. doi: 10.1161/JAHA.121.021037. Epub 2021 Sep 25. J Am Heart Assoc. 2021. PMID: 34569261 Free PMC article.
-
Cardiovascular magnetic resonance of cardiac tumors and masses.World J Cardiol. 2021 Nov 26;13(11):628-649. doi: 10.4330/wjc.v13.i11.628. World J Cardiol. 2021. PMID: 34909128 Free PMC article. Review.
-
Cardiac Adiposity and Arrhythmias: The Role of Imaging.Diagnostics (Basel). 2021 Feb 20;11(2):362. doi: 10.3390/diagnostics11020362. Diagnostics (Basel). 2021. PMID: 33672778 Free PMC article. Review.
-
Lipomatous hypertrophy of the atrial septum - a benign heart anomaly causing unexpected surgical problems: a case report.BMC Cardiovasc Disord. 2018 Jul 28;18(1):152. doi: 10.1186/s12872-018-0892-3. BMC Cardiovasc Disord. 2018. PMID: 30055568 Free PMC article.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
