

Diagnostic timeliness in adolescents and young adults with cancer: a cross-sectional analysis of the BRIGHTLIGHT cohort
- PMID: 29503844
- PMCID: PMC5824669
- DOI: 10.1016/S2352-4642(18)30004-X
Diagnostic timeliness in adolescents and young adults with cancer: a cross-sectional analysis of the BRIGHTLIGHT cohort
Abstract
Background: Adolescents and young adults (AYAs) are thought to experience prolonged intervals to cancer diagnosis, but evidence quantifying this hypothesis and identifying high-risk patient subgroups is insufficient. We aimed to investigate diagnostic timeliness in a cohort of AYAs with incident cancers and to identify factors associated with variation in timeliness.
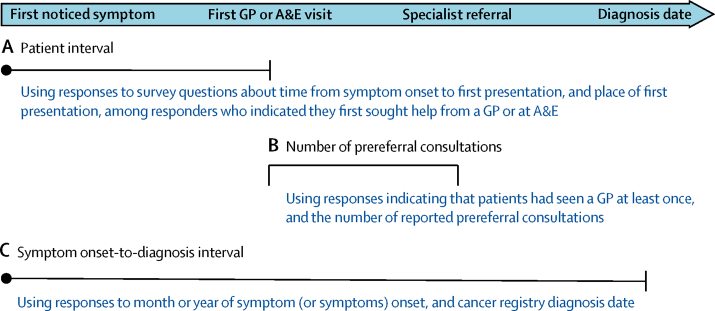
Methods: We did a cross-sectional analysis of the BRIGHTLIGHT cohort, which included AYAs aged 12-24 years recruited within an average of 6 months from new primary cancer diagnosis from 96 National Health Service hospitals across England between July 1, 2012, and April 30, 2015. Participants completed structured, face-to-face interviews to provide information on their diagnostic experience (eg, month and year of symptom onset, number of consultations before referral to specialist care); demographic information was extracted from case report forms and date of diagnosis and cancer type from the national cancer registry. We analysed these data to assess patient interval (time from symptom onset to first presentation to a general practitioner [GP] or emergency department), the number of prereferral GP consultations, and the symptom onset-to-diagnosis interval (time from symptom onset to diagnosis) by patient characteristic and cancer site, and examined associations using multivariable regression models.
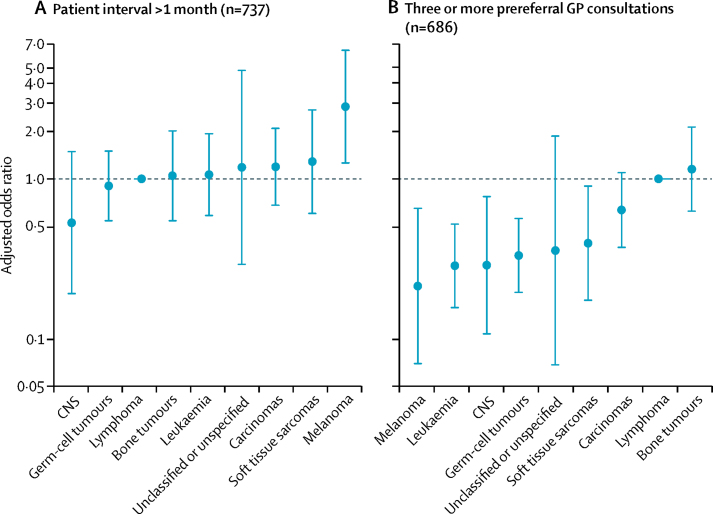
Findings: Of 1114 participants recruited to the BRIGHTLIGHT cohort, 830 completed a face-to-face interview. Among participants with available information, 204 (27%) of 748 had a patient interval of more than a month and 242 (35%) of 701 consulting a general practitioner had three or more prereferral consultations. The median symptom onset-to-diagnosis interval was 62 days (IQR 29-153). Compared with male AYAs, female AYAs were more likely to have three or more consultations (adjusted odds ratio [OR] 1·6 [95% CI 1·1-2·3], p=0·0093) and longer median symptom onset-to-diagnosis intervals (adjusted median interval longer by 24 days [95% CI 11-37], p=0·0005). Patients with lymphoma or bone tumours (adjusted OR 1·2 [95% CI 0·6-2·1] compared with lymphoma) were most likely to have three or more consultations and those with melanoma least likely (0·2 [0·1-0·7] compared with lymphoma). The adjusted median symptom onset-to-diagnosis intervals were longest in AYAs with bone tumours (51 days [95% CI 29-73] longer than for lymphoma) and shortest in those with leukaemia (33 days [17-49] shorter than for lymphoma).
Interpretation: The findings provide a benchmark for diagnostic timeliness in young people with cancer and help to identify subgroups at higher risk of a prolonged diagnostic journey. Further research is needed to understand reasons for these findings and to prioritise and stratify early diagnosis initiatives for AYAs.
Funding: National Institute for Health Research, Teenage Cancer Trust, and Cancer Research UK.
Figures
Comment in
-
Diagnostic timeliness of cancer in adolescents and young adults.Lancet Child Adolesc Health. 2018 Mar;2(3):159-161. doi: 10.1016/S2352-4642(18)30027-0. Epub 2018 Feb 13. Lancet Child Adolesc Health. 2018. PMID: 30169248 No abstract available.
Similar articles
-
Association of Self-reported Presenting Symptoms With Timeliness of Help-Seeking Among Adolescents and Young Adults With Cancer in the BRIGHTLIGHT Study.JAMA Netw Open. 2020 Sep 1;3(9):e2015437. doi: 10.1001/jamanetworkopen.2020.15437. JAMA Netw Open. 2020. PMID: 32880648 Free PMC article.
-
Associations between diagnostic time intervals and health-related quality of life, clinical anxiety and depression in adolescents and young adults with cancer: cross-sectional analysis of the BRIGHTLIGHT cohort.Br J Cancer. 2022 Jun;126(12):1725-1734. doi: 10.1038/s41416-022-01698-6. Epub 2022 Feb 22. Br J Cancer. 2022. PMID: 35190694 Free PMC article.
-
Variation in number of general practitioner consultations before hospital referral for cancer: findings from the 2010 National Cancer Patient Experience Survey in England.Lancet Oncol. 2012 Apr;13(4):353-65. doi: 10.1016/S1470-2045(12)70041-4. Epub 2012 Feb 24. Lancet Oncol. 2012. PMID: 22365494
-
Folic acid supplementation and malaria susceptibility and severity among people taking antifolate antimalarial drugs in endemic areas.Cochrane Database Syst Rev. 2022 Feb 1;2(2022):CD014217. doi: 10.1002/14651858.CD014217. Cochrane Database Syst Rev. 2022. PMID: 36321557 Free PMC article.
-
Specialist cancer services for teenagers and young adults in England: BRIGHTLIGHT research programme.Southampton (UK): NIHR Journals Library; 2021 Nov. Southampton (UK): NIHR Journals Library; 2021 Nov. PMID: 34756846 Free Books & Documents. Review.
Cited by
-
Diagnosed with a Rare Cancer: Experiences of Adult Sarcoma Survivors with the Healthcare System-Results from the SURVSARC Study.Cancers (Basel). 2021 Feb 8;13(4):679. doi: 10.3390/cancers13040679. Cancers (Basel). 2021. PMID: 33567553 Free PMC article.
-
Hodgkin Lymphoma Presenting With Spinal Cord Compression: Challenges for Diagnosis and Initial Management.Pediatr Dev Pathol. 2022 Mar-Apr;25(2):168-173. doi: 10.1177/10935266211033269. Epub 2021 Aug 24. Pediatr Dev Pathol. 2022. PMID: 34428078 Free PMC article. Review.
-
Research priorities for young people with cancer: a UK priority setting partnership with the James Lind Alliance.BMJ Open. 2019 Aug 5;9(8):e028119. doi: 10.1136/bmjopen-2018-028119. BMJ Open. 2019. PMID: 31383701 Free PMC article.
-
Achieving a timely diagnosis for teenagers and young adults with cancer: the ACE "too young to get cancer?" study.BMC Cancer. 2019 Jun 24;19(1):616. doi: 10.1186/s12885-019-5776-0. BMC Cancer. 2019. PMID: 31234813 Free PMC article.
-
Gynecological cancer among adolescents and young adults (AYA).Ann Transl Med. 2020 Mar;8(6):397. doi: 10.21037/atm.2020.02.41. Ann Transl Med. 2020. PMID: 32355841 Free PMC article. Review.
References
-
- Barr RD. Adolescents, young adults, and cancer—the international challenge. Cancer. 2011;117(suppl 10):2245–2249. - PubMed
-
- Fern LA, Lewandowski JA, Coxon KM, Whelan J. Available, accessible, aware, appropriate, and acceptable: a strategy to improve participation of teenagers and young adults in cancer trials. Lancet Oncol. 2014;15:e341–e350. - PubMed
-
- Lethaby CD, Picton S, Kinsey SE, Phillips R, van Laar M, Feltbower RG. A systematic review of time to diagnosis in children and young adults with cancer. Arch Dis Child. 2013;98:349–355. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
