

Influence of proton pump inhibitors on clinical outcomes in coronary heart disease patients receiving aspirin and clopidogrel: A meta-analysis
- PMID: 29504996
- PMCID: PMC5779765
- DOI: 10.1097/MD.0000000000009638
Influence of proton pump inhibitors on clinical outcomes in coronary heart disease patients receiving aspirin and clopidogrel: A meta-analysis
Abstract
Background: Proton pump inhibitors (PPIs) are usually prescribed to protect against gastrointestinal bleeding in patients on dual antiplatelet therapy. This meta-analysis reviewed clinical outcomes in patients taking aspirin and clopidogrel, with and without concomitant PPIs to address concerns of adverse reactions.
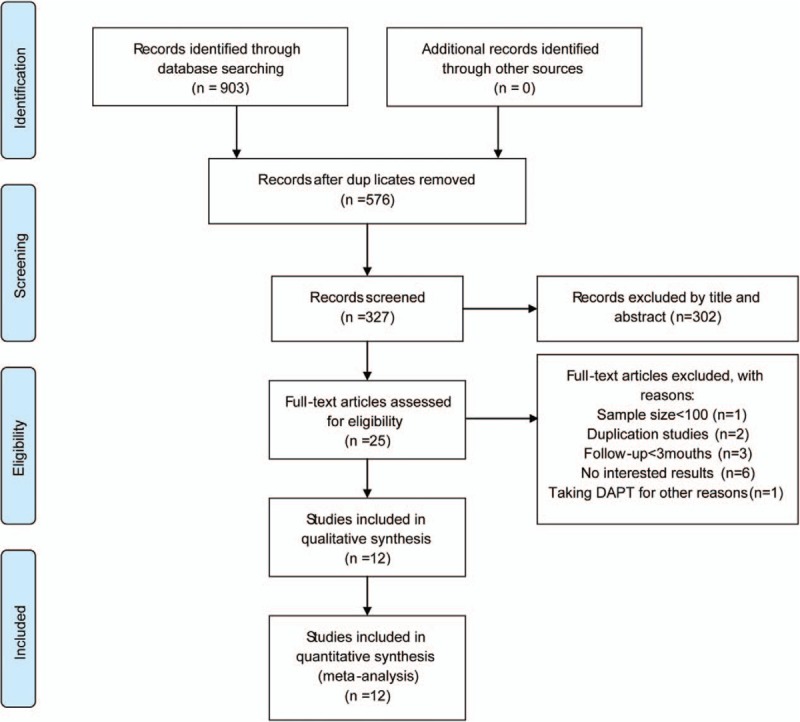
Methods: We searched PubMed, Embase, and the Cochrane Library for articles published between January 1, 2010 and April 11, 2017. The primary end points were major adverse cardiovascular events and gastrointestinal bleeding. Secondary end points were myocardial infarction, stent thrombosis, revascularization, cardiogenic death, and all-cause mortality.
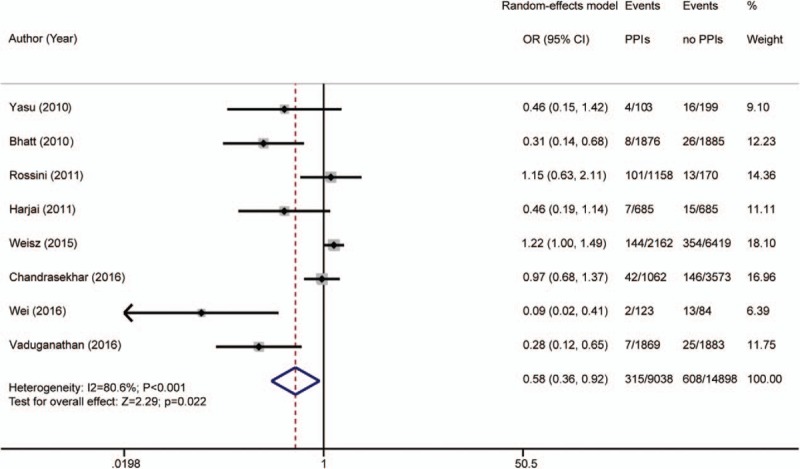
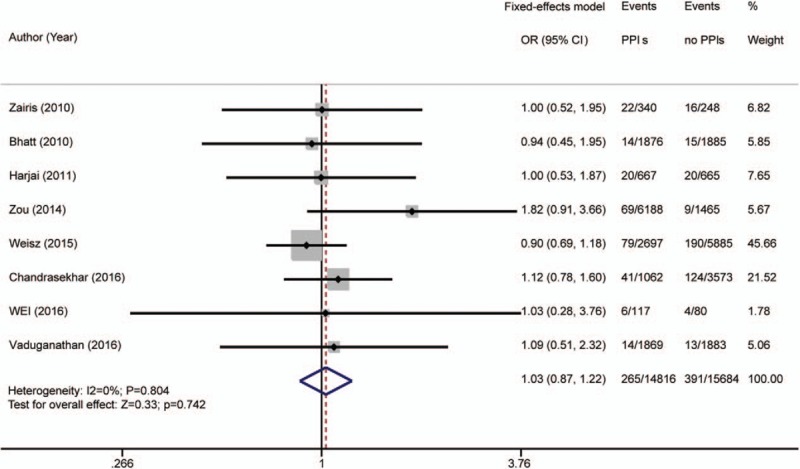
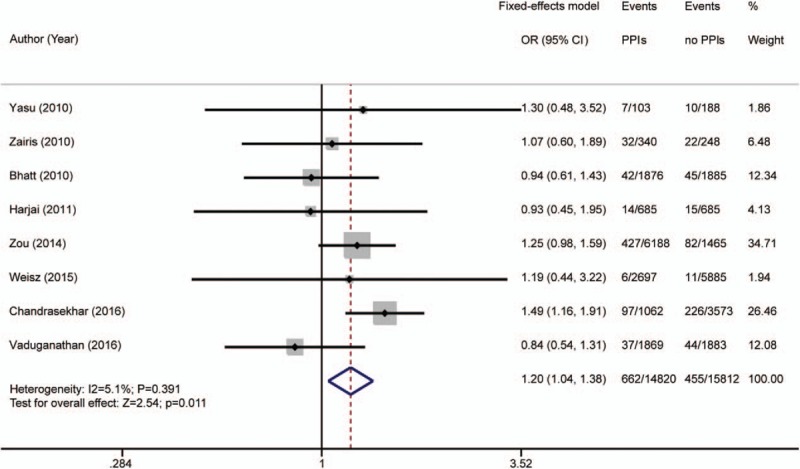
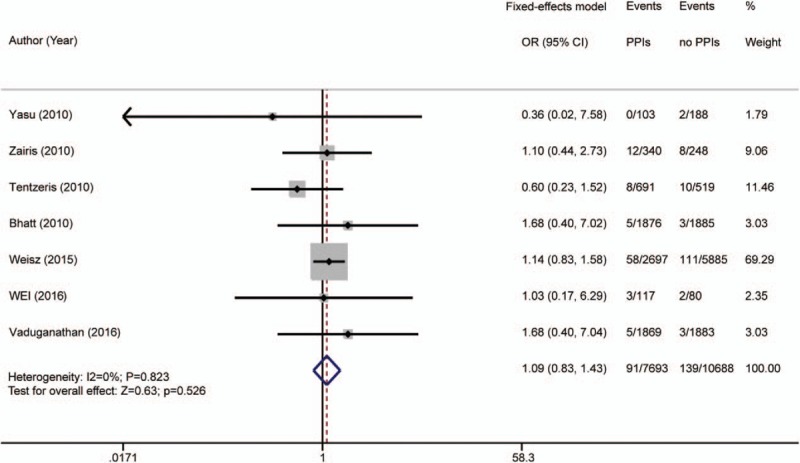
Results: The meta-analysis included 33,492 patients in 4 randomized controlled trials and 8 controlled observational studies. Overall, patients taking PPIs had statistical differences in major adverse cardiovascular events [odds ratio (OR) 1.17 (95% confidence interval [CI] 1.07-1.28); P = .001; I = 28.3%], gastrointestinal bleeding [OR 0.58 (95% CI 0.36-0.92); P = .022; I = 80.6%], stent thrombosis [OR 1.30 (95% CI 1.01-1.68); P = .041; I = 0%], and revascularization [OR 1.20 (95% CI 1.04-1.38); P = .011; I = 5.1%], compared those not taking PPIs. There were no significant differences in myocardial infarction [OR 1.03 (95% CI 0.87-1.22); P = .742; I = 0%], cardiogenic death [OR 1.09 (95% CI 0.83-1.43); P = .526; I = 0%], or all-cause mortality [OR 1.08 (95% CI 0.93-1.25); P = .329; I = 0%).
Conclusions: Among the patients taking aspirin and clopidogrel, the results indicated that the combined use of PPIs increased the rates of major adverse cardiovascular events, stent thrombosis, and revascularization.
Copyright © 2017 The Authors. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors report no conflicts of interest.
Figures




Similar articles
-
Analysis of the Interaction between Clopidogrel, Aspirin, and Proton Pump Inhibitors Using the FDA Adverse Event Reporting System Database.Biol Pharm Bull. 2015;38(5):680-6. doi: 10.1248/bpb.b14-00191. Biol Pharm Bull. 2015. PMID: 25947914
-
Clopidogrel with or without omeprazole in coronary artery disease.N Engl J Med. 2010 Nov 11;363(20):1909-17. doi: 10.1056/NEJMoa1007964. Epub 2010 Oct 6. N Engl J Med. 2010. PMID: 20925534 Clinical Trial.
-
[Meta-analysis on safety and efficacy of dual antiplatelet therapy combining with proton pump inhibitors for patients after percutaneous coronary intervention].Zhonghua Xin Xue Guan Bing Za Zhi. 2019 Feb 24;47(2):129-140. doi: 10.3760/cma.j.issn.0253-3758.2019.02.010. Zhonghua Xin Xue Guan Bing Za Zhi. 2019. PMID: 30818941 Chinese.
-
Drug interaction between clopidogrel and proton pump inhibitors.Pharmacotherapy. 2010 Mar;30(3):275-89. doi: 10.1592/phco.30.3.275. Pharmacotherapy. 2010. PMID: 20180611 Review.
-
Proton pump inhibitors and potential interactions with clopidogrel: an update.Curr Gastroenterol Rep. 2013 Jun;15(6):329. doi: 10.1007/s11894-013-0329-1. Curr Gastroenterol Rep. 2013. PMID: 23695547 Review.
Cited by
-
Effect of Proton Pump Inhibitors on Risks of Upper and Lower Gastrointestinal Bleeding among Users of Low-Dose Aspirin: A Population-Based Observational Study.J Clin Med. 2020 Mar 28;9(4):928. doi: 10.3390/jcm9040928. J Clin Med. 2020. PMID: 32231106 Free PMC article.
-
Proton pump inhibitors and gastroprotection in patients treated with antithrombotic drugs: A cardiologic point of view.World J Cardiol. 2023 Aug 26;15(8):375-394. doi: 10.4330/wjc.v15.i8.375. World J Cardiol. 2023. PMID: 37771340 Free PMC article. Review.
-
Proton Pump Inhibitor Therapy for Eosinophilic Esophagitis: History, Mechanisms, Efficacy, and Future Directions.J Asthma Allergy. 2022 Feb 26;15:281-302. doi: 10.2147/JAA.S274524. eCollection 2022. J Asthma Allergy. 2022. PMID: 35250281 Free PMC article. Review.
-
Management of Nonvariceal Upper Gastrointestinal Bleeding: Guideline Recommendations From the International Consensus Group.Ann Intern Med. 2019 Dec 3;171(11):805-822. doi: 10.7326/M19-1795. Epub 2019 Oct 22. Ann Intern Med. 2019. PMID: 31634917 Free PMC article.
-
Proton pump inhibitor use and mortality in patients with cirrhosis: a meta-analysis of cohort studies.Biosci Rep. 2020 Jun 26;40(6):BSR20193890. doi: 10.1042/BSR20193890. Biosci Rep. 2020. PMID: 32406491 Free PMC article.
References
-
- Levine GN, Bates ER, Bittl JA, et al. 2016 ACC/AHA guideline focused update on duration of dual antiplatelet therapy in patients with coronary artery disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol 2016;68:1082–115. - PubMed
-
- O’Gara PT, Kushner FG, Ascheim DD, et al. 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2013;61:e78–140. - PubMed
-
- Han Y, Xu B, Xu K, et al. Six versus 12 months of dual antiplatelet therapy after implantation of biodegradable polymer sirolimus-eluting stent: randomized substudy of the I-LOVE-IT 2 trial. Circ Cardiovasc Interv 2016;9:e003145. - PubMed
-
- Costa F, Vranckx P, Leonardi S, et al. Impact of clinical presentation on ischaemic and bleeding outcomes in patients receiving 6- or 24-month duration of dual-antiplatelet therapy after stent implantation: a pre-specified analysis from the PRODIGY (Prolonging Dual-Antiplatelet Treatment After Grading Stent-Induced Intimal Hyperplasia) trial. Eur Heart J 2015;36:1242–51. - PubMed
-
- Bhatt DL, Cryer BL, Contant CF, et al. Clopidogrel with or without omeprazole in coronary artery disease. N Engl J Med 2010;363:1909–17. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
