

Fungemia caused by Penicillium marneffei in an immunocompetent patient with COPD: A unique case report
- PMID: 29505004
- PMCID: PMC5779773
- DOI: 10.1097/MD.0000000000009658
Fungemia caused by Penicillium marneffei in an immunocompetent patient with COPD: A unique case report
Abstract
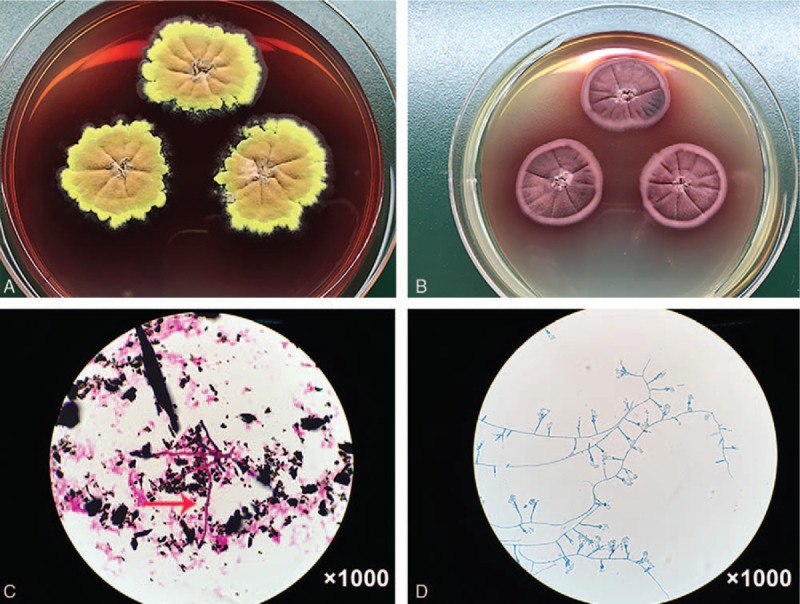
Rationale: This report describes a rare case in Wenzhou city of Zhejiang province that a non-HIV infected male recovering from fungemia caused by Penicillium marneffei (P. marneffei). Interestingly, it's very easy to misdiagnose with aspergillosis, a fungal disease prevalent in Wenzhou, during the whole procedure.
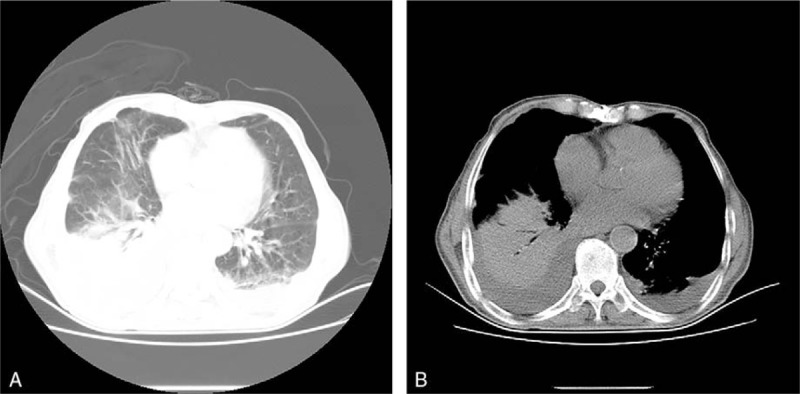
Patient concerns: An 80-year-old Chinese male subject with pre-existing chronic obstructive pulmonary disease (COPD) presented with symptoms of chest tightness and high fever for a month.
Diagnoses: Fungal culture from the blood isolated P marneffei. Naturally, the patient was diagnosed with P marneffei fungemia. However, he was proven serologically to be negative for human immunodeficiency virus (HIV).
Interventions: The patient was treated with voriconazole at 200mg/dL every 12 hours via intravenous administration.
Outcomes: The fever returned to normal and chest tightness disappeared gradually after a week of voriconazole treatment.
Lessons: A high level of clinical suspicion and awareness is necessary for early diagnosis of P marneffei fungemia, especially in elder patients with underlying diseases.
Copyright © 2017 The Authors. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Disseminated Penicillium marneffei infection with fungemia and endobronchial disease in an AIDS patient in China.Med Princ Pract. 2006;15(3):235-7. doi: 10.1159/000092189. Med Princ Pract. 2006. PMID: 16651843
-
Disseminated Penicillium marneffei infection in human immunodeficiency virus-infected children.Pediatr Infect Dis J. 1995 Nov;14(11):935-40. doi: 10.1097/00006454-199511000-00003. Pediatr Infect Dis J. 1995. PMID: 8584358
-
Disseminated Penicillium marneffei infection diagnosed on examination of a peripheral blood smear of a patient with human immunodeficiency virus infection.Clin Infect Dis. 1994 Feb;18(2):246-7. doi: 10.1093/clinids/18.2.246. Clin Infect Dis. 1994. PMID: 8161635
-
Infection due to Penicillium marneffei.Ann Acad Med Singap. 1997 Sep;26(5):701-4. Ann Acad Med Singap. 1997. PMID: 9494682 Review.
-
Disseminated Penicillium marneffei infection as an imported disease in HIV-1 infected patients. Description of two cases and a review of the literature.Neth J Med. 1994 Jan;44(1):18-22. Neth J Med. 1994. PMID: 8202201 Review.
Cited by
-
An Overview of Diagnostic and Management Strategies for Talaromycosis, an Underrated Disease.J Fungi (Basel). 2023 Jun 6;9(6):647. doi: 10.3390/jof9060647. J Fungi (Basel). 2023. PMID: 37367583 Free PMC article. Review.
-
Pulmonary Talaromycosis: A Window into the Immunopathogenesis of an Endemic Mycosis.Mycopathologia. 2021 Oct;186(5):707-715. doi: 10.1007/s11046-021-00570-0. Epub 2021 Jul 6. Mycopathologia. 2021. PMID: 34228343 Free PMC article. Review.
-
Unusual disseminated Talaromyces marneffei infection mimicking lymphoma in a non-immunosuppressed patient in East China: a case report and review of the literature.BMC Infect Dis. 2020 Oct 28;20(1):800. doi: 10.1186/s12879-020-05526-1. BMC Infect Dis. 2020. PMID: 33115429 Free PMC article. Review.
-
A global call for talaromycosis to be recognised as a neglected tropical disease.Lancet Glob Health. 2021 Nov;9(11):e1618-e1622. doi: 10.1016/S2214-109X(21)00350-8. Lancet Glob Health. 2021. PMID: 34678201 Free PMC article. Review.
References
-
- Supparatpinyo K, Sirisanthana T. Disseminated Penicillium marneffei infection diagnosed on examination of a peripheral blood smear of a patient with human immunodeficiency virus infection. Clin Infect Dis 1994;18:246–7. - PubMed
-
- Jiang X, Zhou D. Diagnosis of Penicillium marneffei infection from a blood film. Brit J Haematol 2015;171:670. - PubMed
-
- Uehara M, Sano A, Yarita K, et al. Penicillium marneffei isolated from a Thai AIDS patient with fungemia. Nihon Ishinkin Gakkai Zasshi 2008;49:205–9. - PubMed
-
- De Monte A, Risso K, Normand AC, et al. Chronic pulmonary penicilliosis due to Penicillium marneffei: late presentation in a French traveler. J Travel Med 2014;21:292–4. - PubMed
-
- Capponi M, Segretain G, Sureau P. Penicillosis from Rhizomys sinensis. Bull Soc Pathol Exot Filiales 1956;49:418–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
