

Molecular Classification of Grade 3 Endometrioid Endometrial Cancers Identifies Distinct Prognostic Subgroups
- PMID: 29505428
- PMCID: PMC5893364
- DOI: 10.1097/PAS.0000000000001020
Molecular Classification of Grade 3 Endometrioid Endometrial Cancers Identifies Distinct Prognostic Subgroups
Abstract
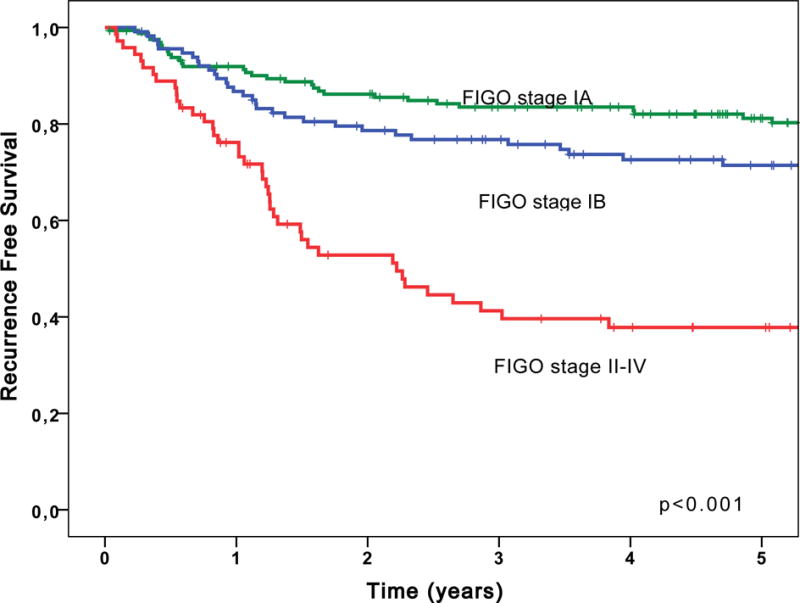
Our aim was to investigate whether molecular classification can be used to refine prognosis in grade 3 endometrial endometrioid carcinomas (EECs). Grade 3 EECs were classified into 4 subgroups: p53 abnormal, based on mutant-like immunostaining (p53abn); MMR deficient, based on loss of mismatch repair protein expression (MMRd); presence of POLE exonuclease domain hotspot mutation (POLE); no specific molecular profile (NSMP), in which none of these aberrations were present. Overall survival (OS) and recurrence-free survival (RFS) rates were compared using the Kaplan-Meier method (Log-rank test) and univariable and multivariable Cox proportional hazard models. In total, 381 patients were included. The median age was 66 years (range, 33 to 96 y). Federation Internationale de Gynecologie et d'Obstetrique stages (2009) were as follows: IA, 171 (44.9%); IB, 120 (31.5%); II, 24 (6.3%); III, 50 (13.1%); IV, 11 (2.9%). There were 49 (12.9%) POLE, 79 (20.7%) p53abn, 115 (30.2%) NSMP, and 138 (36.2%) MMRd tumors. Median follow-up of patients was 6.1 years (range, 0.2 to 17.0 y). Compared to patients with NSMP, patients with POLE mutant grade 3 EEC (OS: hazard ratio [HR], 0.36 [95% confidence interval, 0.18-0.70]; P=0.003; RFS: HR, 0.17 [0.05-0.54]; P=0.003) had a significantly better prognosis; patients with p53abn tumors had a significantly worse RFS (HR, 1.73 [1.09-2.74]; P=0.021); patients with MMRd tumors showed a trend toward better RFS. Estimated 5-year OS rates were as follows: POLE 89%, MMRd 75%, NSMP 69%, p53abn 55% (Log rank P=0.001). Five-year RFS rates were as follows: POLE 96%, MMRd 77%, NSMP 64%, p53abn 47% (P=0.000001), respectively. In a multivariable Cox model that included age and Federation Internationale de Gynecologie et d'Obstetrique stage, POLE and MMRd status remained independent prognostic factors for better RFS; p53 status was an independent prognostic factor for worse RFS. Molecular classification of grade 3 EECs reveals that these tumors are a mixture of molecular subtypes of endometrial carcinoma, rather than a homogeneous group. The addition of molecular markers identifies prognostic subgroups, with potential therapeutic implications.
Conflict of interest statement
Figures



References
-
- NIH National Cancer Institute. Surveillance Epidemiology, and End Results Program. (Cancer Statistics).Cancer Stat Facts: Endometrial Cancer. 2017 Available at: http://seer.cancer.gov/statfacts/html/corp.html. Accessed 10/12/2017.
-
- Proctor L, Pradhan M, Leung S, et al. Assessment of DNA Ploidy in the ProMisE molecular subgroups of endometrial cancer. Gynecol Oncol. 2017;146:596–602. - PubMed
-
- Stelloo E, Bosse T, Nout RA, et al. Refining prognosis and identifying targetable pathways for high-risk endometrial cancer; a TransPORTEC initiative. Mod Pathol. 2015;28:836–844. - PubMed
-
- Stelloo E, Nout RA, Osse EM, et al. Improved Risk Assessment by Integrating Molecular and Clinicopathological Factors in Early-stage Endometrial Cancer-Combined Analysis of the PORTEC Cohorts. Clin Cancer Res. 2016;22:4215–4224. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
