

Survival benefits of pelvic lymphadenectomy versus pelvic and para-aortic lymphadenectomy in patients with endometrial cancer: A meta-analysis
- PMID: 29505525
- PMCID: PMC5943115
- DOI: 10.1097/MD.0000000000009520
Survival benefits of pelvic lymphadenectomy versus pelvic and para-aortic lymphadenectomy in patients with endometrial cancer: A meta-analysis
Abstract
Background: Despite that pelvic and para-aortic lymphadenectomy (PPaLND) is recommended as part of accurate surgical staging by International Federation of Gynecology and Obstetrics (FIGO) in endometrial cancer, the impact of para-aortic lymphadenectomy on survival remains controversial. The aim of this work is to evaluate the survival benefits or risks in endometrial cancer patients who underwent surgical staging with or without para-aortic lymphadenectomy using meta-analysis.
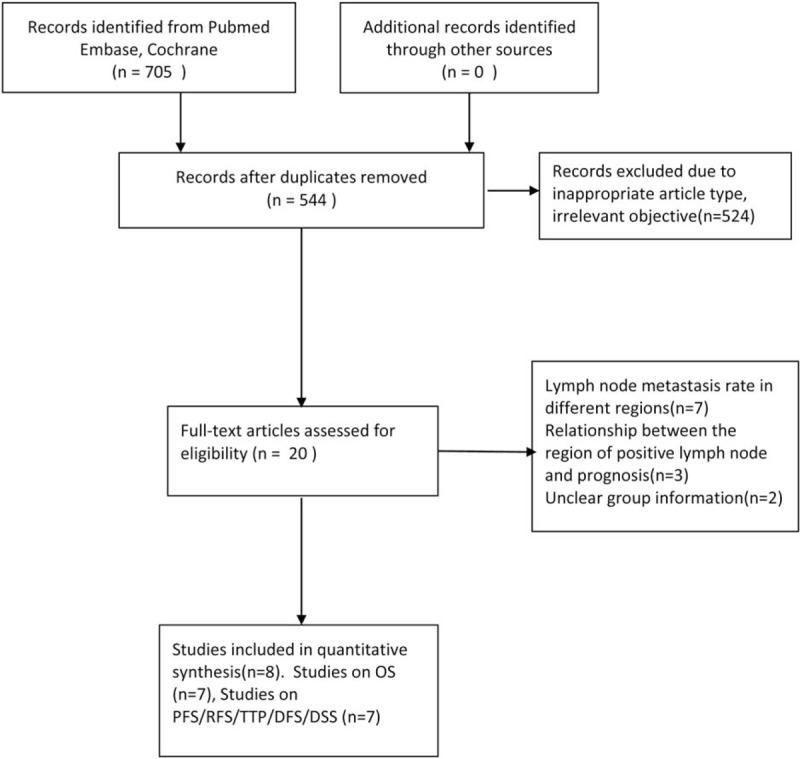
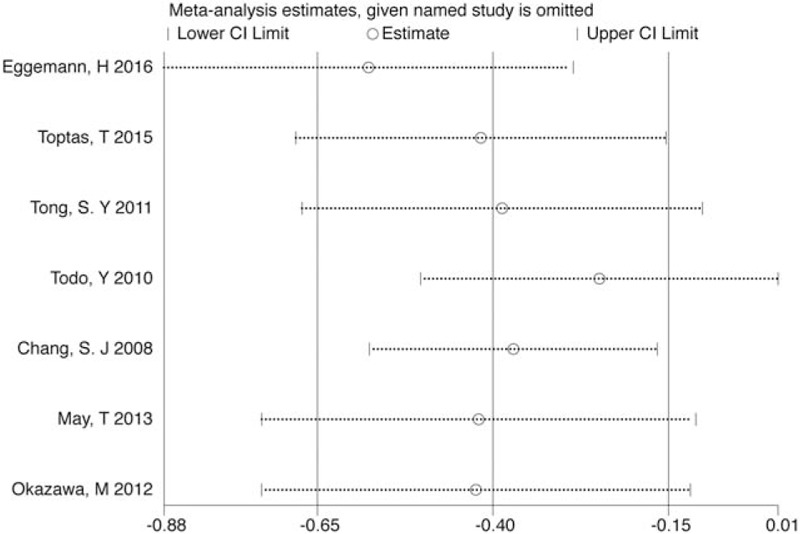
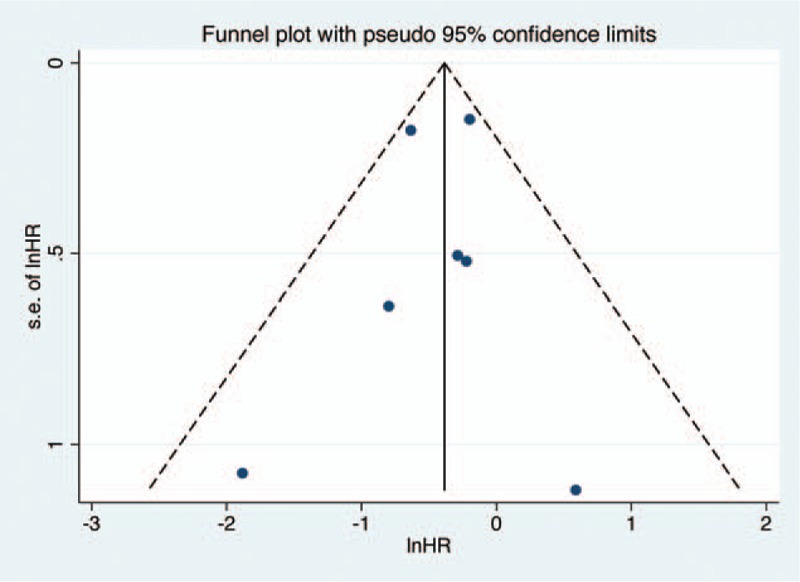
Methods: Literature search was undertaken using PubMed, Embase, and Cochrane Library databases for relevant articles published between January 1, 1990, and January 1, 2017, without language restriction. The primary outcome was overall survival (OS); progression-free survival (PFS)/recurrence-free survival (RFS)/disease-free survival (DFS)/disease-related survival (DRS) was also analyzed. Subgroup analysis and sensitivity analysis were conducted to investigate the source of heterogeneity. Quality assessments were performed by Newcastle-Ottawa Quality Assessment Scale (NOS). Publication bias was evaluated by using Begg and Egger tests. The hazard ratio (HR) was pooled with random-effects or fixed-effects model as appropriate.
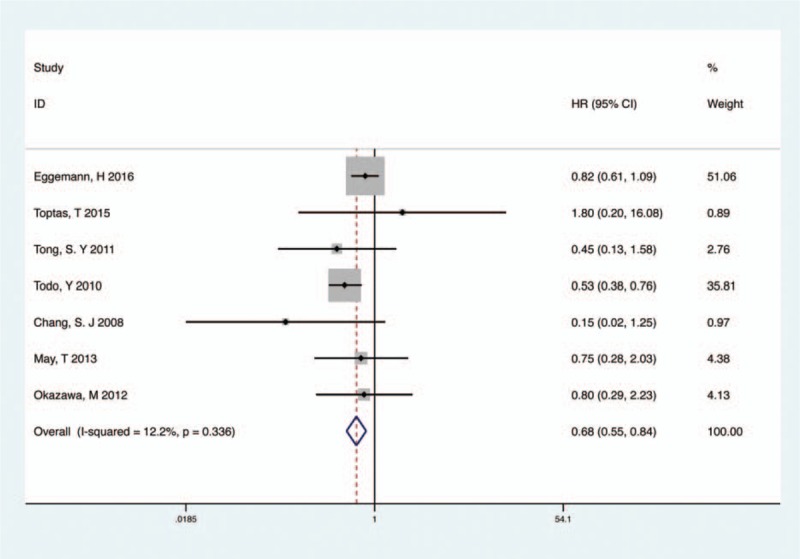
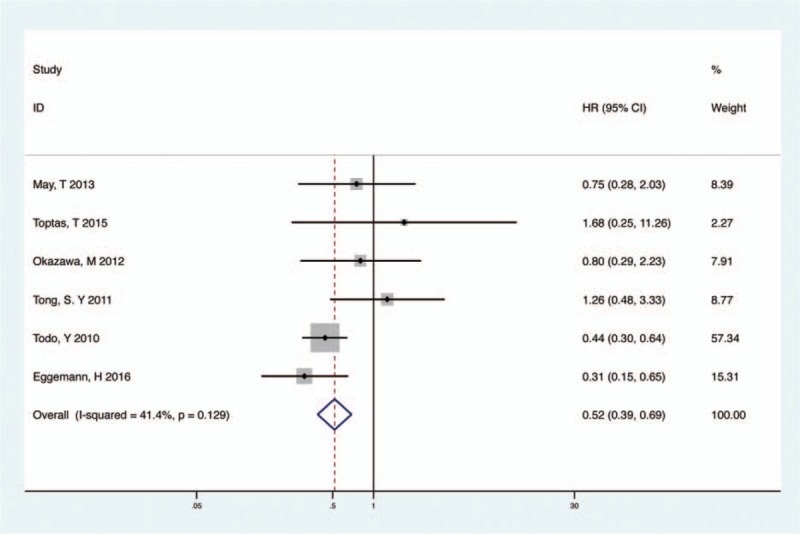
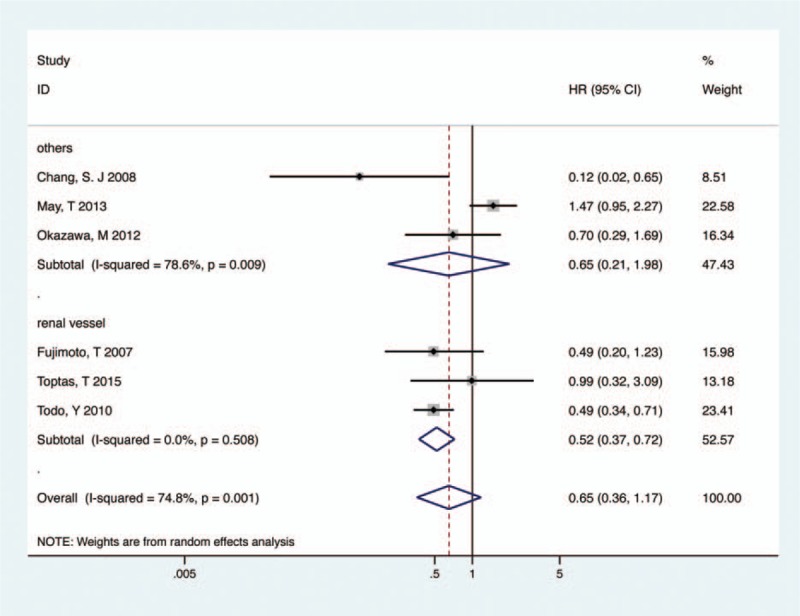
Results: Eight studies with a total of 2793 patients were included. OS was significantly longer in PPaLND group than in pelvic lymphadenectomy (PLND) group for patients with endometrial cancer [HR 0.68; 95% confidence interval (CI) 0.55-0.84, P < .001, I = 12.2%]. Subgroup analysis by recurrence risk explored the same association in patients at intermediate- or high-risk (HR 0.52; 95% CI 0.39-0.69, P < .001, I = 41.4%), but not for low-risk patients (HR 0.48; 95% CI 0.21-1.08, P = .077, I = 0). PPaLND with systematic resection of all para-aortic nodes up to renal vein also improved PFS/RFS/DFS/DRS, compared with PLND (HR 0.52, 95% CI 0.37-0.72, P < .001, I = 0). No publication bias was observed among included studies.
Conclusion: PPaLND is associated with favorable survival outcomes in endometrial cancer patients with intermediate- or high-risk of recurrence compared with PLND, particularly with regards to OS. PPaLND with systematic resection of all para-aortic nodes up to renal vein also improve PFS compared with PLND. Further large-scale randomized clinical trials are required to validate our findings.
Copyright © 2017 The Authors. Published by Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015;136:E359–86. - PubMed
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin 2017;67:7–30. - PubMed
-
- Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide: IARC CancerBase No. 11. 2013;Lyon, France: International Agency for Research on Cancer, Available from: http://globocan.iarc.fr, accessed March 1, 2014.
-
- Shepherd JH. Revised FIGO staging for gynaecological cancer. Br J Obstet Gynaecol 1989;96:889–92. - PubMed
-
- Pecorelli S. Revised FIGO staging for carcinoma of the vulva, cervix, and endometrium. Int J Gynaecol Obstet 2009;105:103–4. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
