

Impact of contraceptive initiation on vaginal microbiota
- PMID: 29505773
- PMCID: PMC5990849
- DOI: 10.1016/j.ajog.2018.02.017
Impact of contraceptive initiation on vaginal microbiota
Erratum in
-
June 2018 (vol. 218, no. 6, pages 622.e1-10).Am J Obstet Gynecol. 2021 Oct;225(4):434. doi: 10.1016/j.ajog.2021.01.034. Epub 2021 Mar 30. Am J Obstet Gynecol. 2021. PMID: 33810848 Free PMC article. No abstract available.
Abstract
Background: Data evaluating the impact of contraceptives on the vaginal microbiome are limited and inconsistent.
Objective: We hypothesized that women initiating copper intrauterine device use would have increased bacterial vaginosis and bacterial vaginosis-associated microbes with use compared to women initiating and using hormonal contraceptive methods.
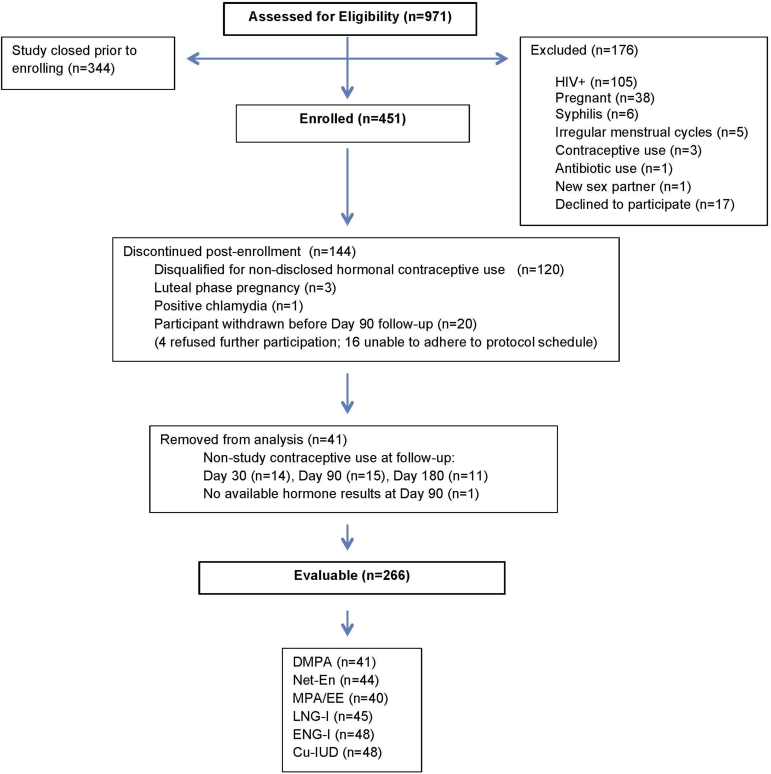
Study design: Vaginal swabs (N = 1047 from 266 participants seeking contraception) for Nugent score determination of bacterial vaginosis and quantitative polymerase chain reaction analyses for assessment of specific microbiota were collected from asymptomatic, healthy women aged 18-35 years in Harare, Zimbabwe, who were confirmed to be free of nonstudy hormones by mass spectrometry at each visit. Contraception was initiated with an injectable (depot medroxyprogesterone acetate [n = 41], norethisterone enanthate [n = 44], or medroxyprogesterone acetate and ethinyl estradiol [n = 40]), implant (levonorgestrel [n = 45] or etonogestrel [n = 48]), or copper intrauterine device (n = 48) and repeat vaginal swabs were collected after 30, 90, and 180 days of continuous use. Self-reported condom use was similar across all arms at baseline. Quantitative polymerase chain reaction was used to detect Lactobacillus crispatus, L jensenii, L gasseri/johnsonii group, L vaginalis, L iners, Gardnerella vaginalis, Atopobium vaginae, and Megasphaera-like bacterium phylotype I from swabs. Modified Poisson regression and mixed effects linear models were used to compare marginal prevalence and mean difference in quantity (expressed as gene copies/swab) prior to and during contraceptive use.
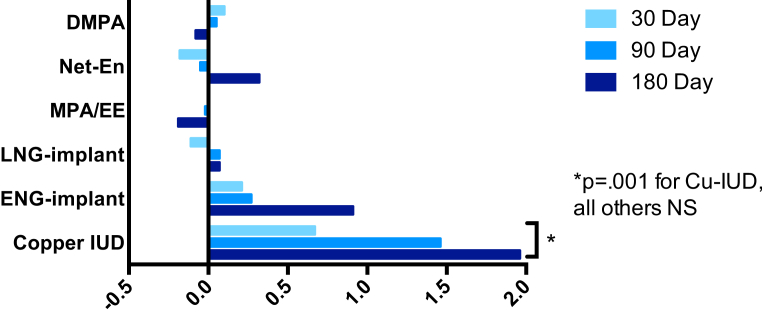
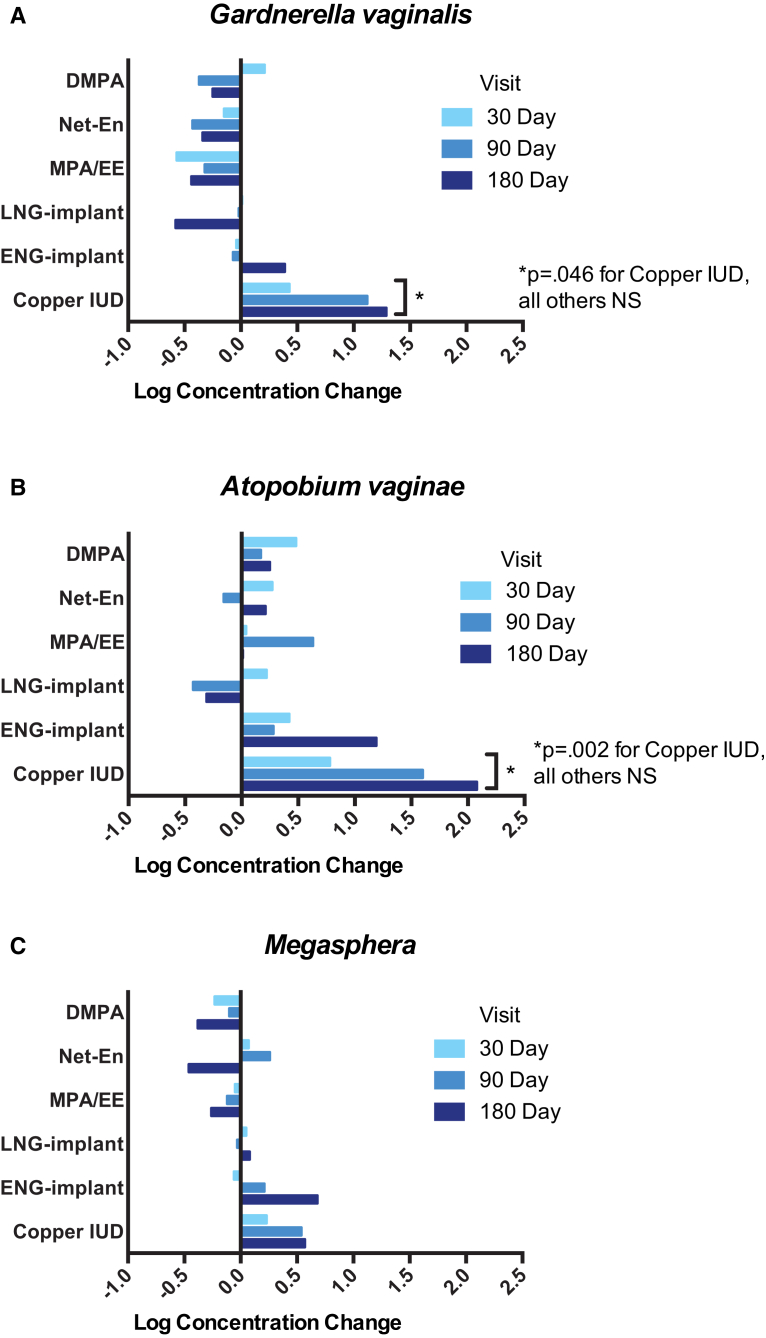
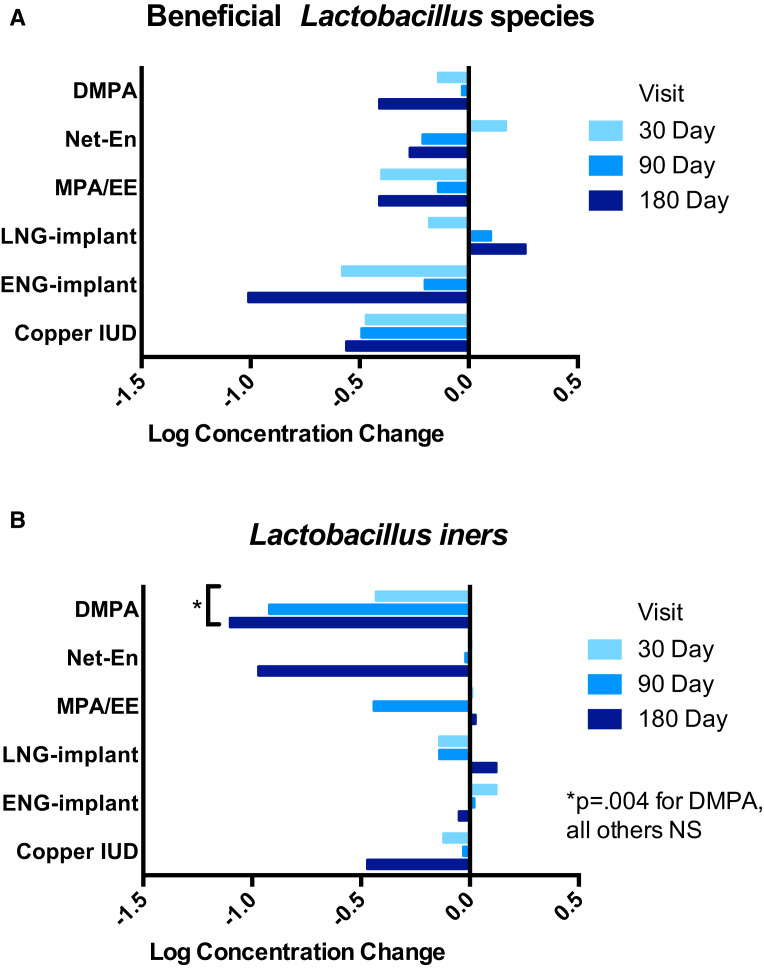
Results: Bacterial vaginosis prevalence increased in women initiating copper intrauterine devices from 27% at baseline, 35% at 30 days, 40% at 90 days, and 49% at 180 days (P = .005 compared to marginal prevalence at enrollment). Women initiating hormonal methods had no change in bacterial vaginosis prevalence over 180 days. The mean increase in Nugent score was 1.2 (95% confidence interval, 0.5-2.0; P = .001) in women using copper intrauterine devices. Although the frequency and density of beneficial lactobacilli did not change among intrauterine device users over 6 months, there was an increase in the log concentration of G vaginalis (4.7, 5.2, 5.8, 5.9; P = .046) and A vaginae (3.0, 3.8, 4.6, 5.1; P = .002) between baseline and 30, 90, and 180 days after initiation. Among other contraceptive groups, women using depot medroxyprogesterone acetate had decreased L iners (mean decrease log concentration = 0.8; 95% confidence interval, 0.3-1.5; P = .004) and there were no significant changes in beneficial Lactobacillus species over 180 days regardless of contraceptive method used.
Conclusion: Copper intrauterine device use may increase colonization by bacterial vaginosis-associated microbiota, resulting in increased prevalence of bacterial vaginosis. Use of most hormonal contraception does not alter vaginal microbiota.
Keywords: bacterial vaginosis; hormonal contraception; intrauterine device; lactobacilli; vaginal microbiota.
Copyright © 2018 The Author(s). Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Wiesenfeld H.C., Hillier S.L., Krohn M.A., Landers D.V., Sweet R.L. Bacterial vaginosis is a strong predictor of Neisseria gonorrhoeae and Chlamydia trachomatis infection. Clin Infect Dis. 2003;36:663–668. - PubMed
-
- Gallo M.F., Macaluso M., Warner L. Bacterial vaginosis, gonorrhea, and chlamydial infection among women attending a sexually transmitted disease clinic: a longitudinal analysis of possible causal links. Ann Epidemiol. 2012;22:213–220. - PubMed
-
- Taha T.E., Hoover D.R., Dallabetta G.A. Bacterial vaginosis and disturbances of vaginal flora: association with increased acquisition of HIV. AIDS. 1998;12:1699–1706. - PubMed
