

Hospital readmissions with acute infectious diseases in New Zealand children < 2 years of age
- PMID: 29506511
- PMCID: PMC5838880
- DOI: 10.1186/s12887-018-1079-x
Hospital readmissions with acute infectious diseases in New Zealand children < 2 years of age
Abstract
Background: Infectious diseases are the leading cause of hospital admissions in young children. Hospitalisation with an infectious disease is a recurrent event for some children. Our objective was to describe risk factors for infectious disease readmission following hospital admission with an infectious disease in the first two years of life.
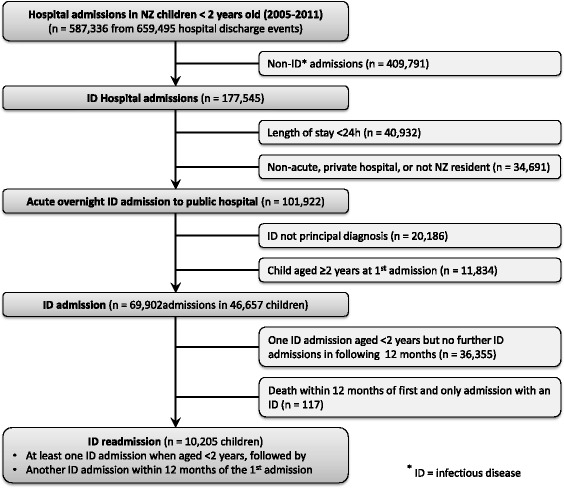
Methods: We performed a national cohort study of New Zealand children, born 2005-2009, with an infectious disease admission before age 24 months. Children readmitted with an infectious disease within 12 months of the first infectious disease admission were identified. Every infectious disease admission was categorised as a respiratory, enteric, skin and soft tissue, urinary or other infection. Independent associations of demographic and child health factors with infectious disease readmission were determined using multiple variable logistic regression.
Results: From 2005 to 2011, there were 69,902 infectious disease admissions for 46,657 children less than two years old. Of these 46,657 children, 10,205 (22%) had at least one infectious disease readmission within 12 months of their first admission. The first infectious disease admission was respiratory (54%), enteric (15%), skin or soft tissue (7%), urinary (4%) or other (20%). Risk of infectious disease readmission was increased if the first infectious disease admission was respiratory (OR = 1.87, 95% CI 1.78-1.95) but not if it was in any other infectious disease category. Risk factors for respiratory infectious disease readmission were male gender, Pacific or Māori ethnicity, greater household deprivation, presence of a complex chronic condition, or a first respiratory infectious disease admission during autumn or of ≥3 days duration. Fewer factors (younger age, male gender, presence of a complex chronic condition) were associated with enteric infection readmission. The presence of a complex chronic condition was the only factor associated with urinary tract infection readmission and none of the factors were associated with skin or soft tissue infection readmission.
Conclusions: In children less than two years old, infectious disease readmission risk is increased if the first infectious disease admission is a respiratory infectious disease but not if it is another infectious disease category. Risk factors for respiratory infectious disease readmission are different from those for other infectious disease readmissions.
Keywords: Child preschool; Cohort studies; Diarrhea; Hospitalization; Infant; Patient readmission; Respiratory tract infections; Skin and soft tissue infections; Urinary tract infections.
Conflict of interest statement
Ethics approval and consent to participate
The study protocol was reviewed by the NZ Health and Disabilities Ethics Committee, with the ethics committee determining that ethical approval was not required. The NZ Ministry of Health granted data access, providing data with encrypted NHI numbers to maintain patient anonymity.
Consent for publication
Not applicable.
Competing interests
The authors have no competing interests to declare.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
-
- Kassebaum N, Kyu HH, Zoeckler L, Olsen HE, Thomas K, Pinho C, Bhutta ZA, Dandona L, Ferrari A, Ghiwot TT, et al. Child and adolescent health from 1990 to 2015: findings from the global burden of diseases, injuries, and risk factors 2015 study. JAMA Pediatr. 2017;171(6):573–592. doi: 10.1001/jamapediatrics.2017.0250. - DOI - PMC - PubMed
-
- Baker MG, Barnard LT, Kvalsvig A, Verrall A, Zhang J, Keall M, Wilson N, Wall T, Howden-Chapman P. Increasing incidence of serious infectious diseases and inequalities in New Zealand: a national epidemiological study. Lancet. 2012;379(9821):1112–1119. doi: 10.1016/S0140-6736(11)61780-7. - DOI - PubMed
-
- Craig E, Adams J, Oben G, Reddington A, Wicken A, Simpson J. Department of Women’s and Children’s Health at the University of Otago’s Dunedin School of Medicine: University of Otago. 2013. Service NCaYE: The Health Status of Children and Young People in New Zealand.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
