

Evaluation of community-level interventions to increase early initiation of antenatal care in pregnancy: protocol for the Community REACH study, a cluster randomised controlled trial with integrated process and economic evaluations
- PMID: 29506563
- PMCID: PMC5838929
- DOI: 10.1186/s13063-018-2526-6
Evaluation of community-level interventions to increase early initiation of antenatal care in pregnancy: protocol for the Community REACH study, a cluster randomised controlled trial with integrated process and economic evaluations
Abstract
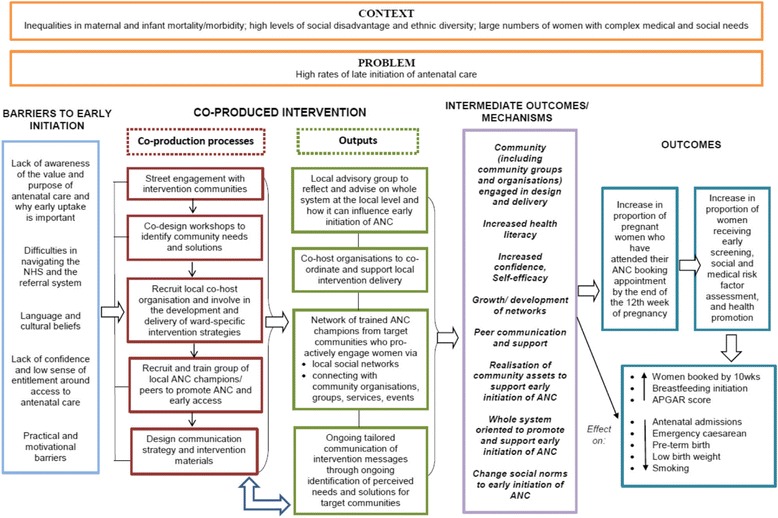
Background: The provision of high-quality maternity services is a priority for reducing inequalities in health outcomes for mothers and infants. Best practice includes women having their initial antenatal appointment within the first trimester of pregnancy in order to provide screening and support for healthy lifestyles, well-being and self-care in pregnancy. Previous research has identified inequalities in access to antenatal care, yet there is little evidence on interventions to improve early initiation of antenatal care. The Community REACH trial will assess the effectiveness and cost-effectiveness of engaging communities in the co-production and delivery of an intervention that addresses this issue.
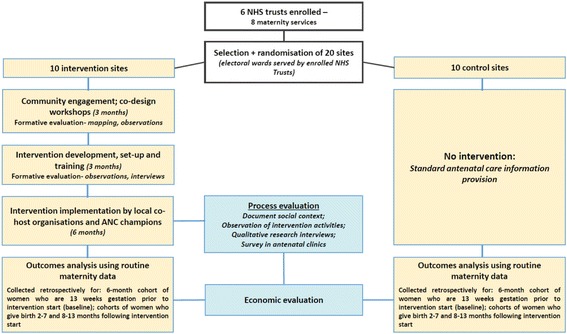
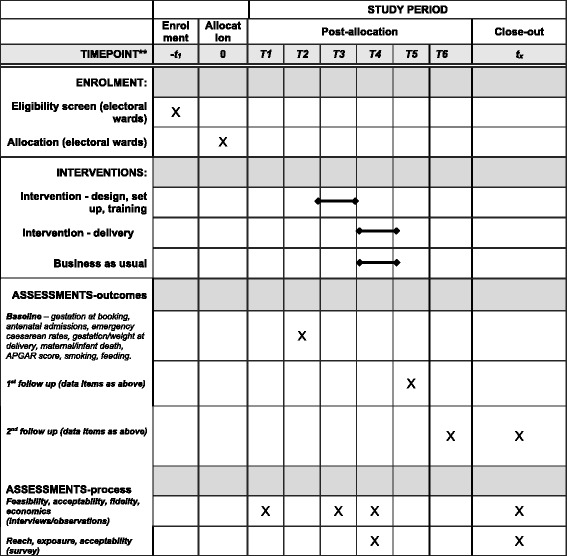
Methods/design: The study design is a matched cluster randomised controlled trial with integrated process and economic evaluations. The unit of randomisation is electoral ward. The intervention will be delivered in 10 wards; 10 comparator wards will have normal practice. The primary outcome is the proportion of pregnant women attending their antenatal booking appointment by the 12th completed week of pregnancy. This and a number of secondary outcomes will be assessed for cohorts of women (n = approximately 1450 per arm) who give birth 2-7 and 8-13 months after intervention delivery completion in the included wards, using routinely collected maternity data. Eight hospitals commissioned to provide maternity services in six NHS trusts in north and east London and Essex have been recruited to the study. These trusts will provide anonymised routine data for randomisation and outcomes analysis. The process evaluation will examine intervention implementation, acceptability, reach and possible causal pathways. The economic evaluation will use a cost-consequences analysis and decision model to evaluate the intervention. Targeted community engagement in the research process was a priority.
Discussion: Community REACH aims to increase early initiation of antenatal care using an intervention that is co-produced and delivered by local communities. This pragmatic cluster randomised controlled trial, with integrated process and economic evaluation, aims to rigorously assess the effectiveness of this public health intervention, which is particularly complex due to the required combination of standardisation with local flexibility. It will also answer questions about scalability and generalisability.
Trial registration: ISRCTN registry: registration number 63066975 . Registered on 18 August 2015.
Keywords: Access to care; Antenatal care; Cluster randomised controlled trial; Co-production; Community engagement; Maternity.
Conflict of interest statement
Ethics approval and consent to participate
The study has been approved by the NHS Health Research Authority National Research Ethics Committee North East-York (27 March 2015, ref.15/NE/0106) and the appropriate permissions for all the participating sites secured. All information collected during the trial will be kept confidential and adhere to the 1998 Data Protection Act.
There is no individual consent process for the outcomes evaluation due to the reliance on anonymous routine data. For the observation of community co-design workshops, participants were informed before the workshop began, that the researcher would not record any personal or identifiable data concerning anyone in attendance. Remaining in the workshop was interpreted as participants giving consent to the researcher making non-identifiable notes of the workshop processes. All potential survey and interview participants will be taken through information and consent procedures with verbal and written information provided before written consent is requested. Potential participants will be given adequate time to consider whether or not they want to participate – with contact details given to the research team should they want more time for this. Bilingual research assistants or health care interpreters (in antenatal clinics) will be included in the informed consent and data collection processes to provide language support where necessary.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Marmot M, Allen J, Goldblatt P, et al. Fair society, healthy lives: strategic review of health inequalities in England post 2010. London: Marmot Review Team; 2010.
-
- Oakley L, Gray R, Kurinczuk JJ, Brocklehurst P, Hollowell J. A systematic review of the effectiveness of interventions to increase the early initiation of antenatal care in socially disadvantaged and vulnerable women. Oxford: National Perinatal Epidemiology Unit; 2009.
-
- National Institute for Health and Clinical Excellence . Antenatal Care for Uncomplicated Pregnancies: NICE guidelines [CG62] Manchester: National Institute for Health and Clinical Excellence; 2008. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
