

Laparoscopic inguinal ligament suspension versus laparoscopic sacrocolpopexy in the treatment of pelvic organ prolapse: study protocol for a randomized controlled trial
- PMID: 29506566
- PMCID: PMC5838885
- DOI: 10.1186/s13063-018-2494-x
Laparoscopic inguinal ligament suspension versus laparoscopic sacrocolpopexy in the treatment of pelvic organ prolapse: study protocol for a randomized controlled trial
Abstract
Background: Pelvic organ prolapse (POP) is a common health problem. The lifetime risk of undergoing surgery for prolapse is 11%. POP significantly affects the effects on quality of life and activities of daily living. Laparoscopic sacrocolpopexy (LSC) has been viewed as the gold standard treatment for women with POP who desire reconstructive surgery. However, LSC is associated with technical difficulties, resulting in a long learning curve and operative time. Recently, our team introduced a new laparoscopic technique of inguinal ligament suspension (LILS) and had confirmed its safety and efficacy in treating vaginal vault prolapse. As a new surgical technique for POP, a prospective randomized controlled trial comparing the LILS with the standard technique of LSC is necessary. Therefore, we will conduct a trial.
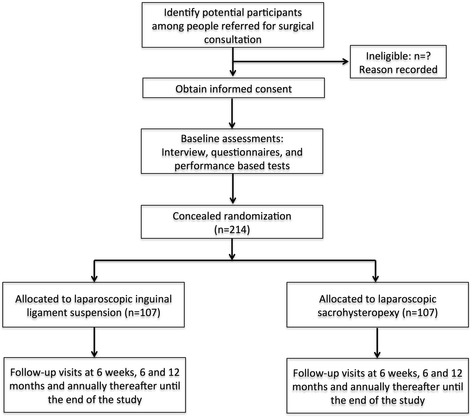
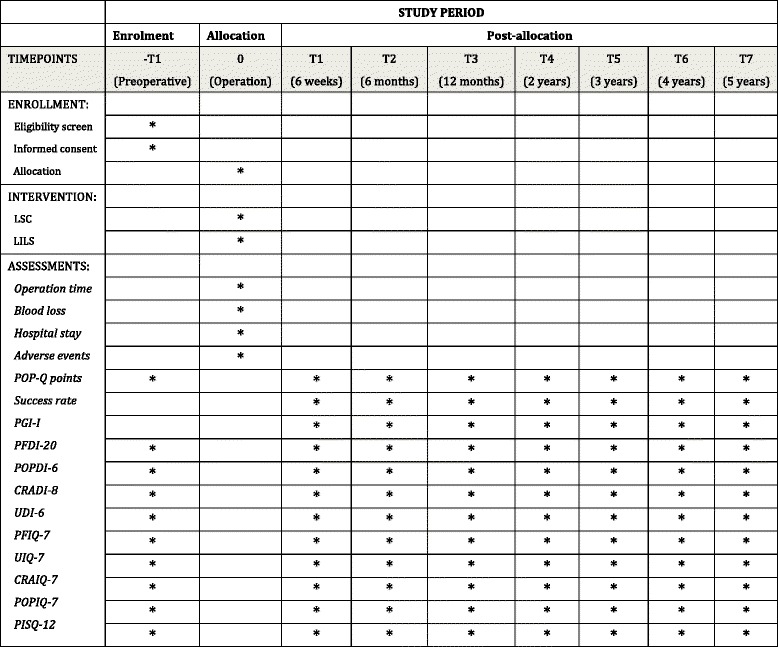
Methods: The trial is a randomized controlled trial. It compares LILS with LSC in women with stage 2 or higher uterine prolapse. The primary outcomes of this study are perioperative parameters, including surgical time, blood loss, intraoperative complications, and hospital stay as well as surgical anatomical results using the pelvic organ prolapse questionnaire (POP-Q) classification at 6 weeks, 6 months, 12 months, and annually till 5 years after surgery. Secondary outcomes are subjective improvement in urogenital symptoms and quality of life, postoperative complications, postoperative recovery, sexual functioning, and cost-effectiveness at each follow-up point. Validated questionnaires will be used and the data will be analyzed according to the intention-to-treat principle. Based on an objective success rate of 90%, a noninferiority margin of 15%, and a dropout of 20%, 107 patients are needed in each arm to prove the hypothesis with a 95% confidence interval.
Discussion: The trial is a randomized controlled, multicenter, noninferiority trial that will provide evidence whether the efficacy and safety of LILS is noninferior to LSC in women with symptomatic stage 2 or higher uterine prolapse.
Trial registration: China Trial Register (CTR): ChiCTR-INR-15007408 . Registered on 9 November 2015.
Keywords: Laparoscopic inguinal ligament suspension; Laparoscopic sacrohysteropexy; Pelvic organ prolapse.
Conflict of interest statement
Ethics approval and consent to participate
The trial has been approved by the Medical Ethics Committee of Shanghai First Infant and Maternity Hospital and the local ethics committees of the participating centers (KS1513). Written informed consent will be obtained and documented for all study participants.
Consent for publication
The authors declare that they agree with publication.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Hysteropexy in the treatment of uterine prolapse stage 2 or higher: a multicenter randomized controlled non-inferiority trial comparing laparoscopic sacrohysteropexy with vaginal sacrospinous hysteropexy (LAVA-trial, study protocol).BMC Womens Health. 2014 Sep 17;14:112. doi: 10.1186/1472-6874-14-112. BMC Womens Health. 2014. PMID: 25231240 Free PMC article. Clinical Trial.
-
Laparoscopic sacrocolpopexy versus vaginal sacrospinous fixation for vaginal vault prolapse, a randomized controlled trial: SALTO-2 trial, study protocol.BMC Womens Health. 2017 Jul 26;17(1):52. doi: 10.1186/s12905-017-0402-2. BMC Womens Health. 2017. PMID: 28747206 Free PMC article. Clinical Trial.
-
Laparoscopic inguinal ligament suspension with uterine preservation for pelvic organ prolapse: A retrospective cohort study.Int J Surg. 2018 Jun;54(Pt A):28-34. doi: 10.1016/j.ijsu.2018.04.020. Epub 2018 Apr 16. Int J Surg. 2018. PMID: 29673691
-
Guideline No. 413: Surgical Management of Apical Pelvic Organ Prolapse in Women.J Obstet Gynaecol Can. 2021 Apr;43(4):511-523.e1. doi: 10.1016/j.jogc.2021.02.001. Epub 2021 Feb 3. J Obstet Gynaecol Can. 2021. PMID: 33548503
-
The current status of laparoscopic sacrocolpopexy: a review.Eur Urol. 2009 May;55(5):1089-103. doi: 10.1016/j.eururo.2009.01.048. Epub 2009 Feb 4. Eur Urol. 2009. PMID: 19201521 Review.
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
