

Fine-scale spatial and temporal variation of clinical malaria incidence and associated factors in children in rural Malawi: a longitudinal study
- PMID: 29506570
- PMCID: PMC5839004
- DOI: 10.1186/s13071-018-2730-y
Fine-scale spatial and temporal variation of clinical malaria incidence and associated factors in children in rural Malawi: a longitudinal study
Abstract
Background: Spatio-temporal variations in malaria burden are currently complex and costly to measure, but are important for decision-making. We measured the spatio-temporal variation of clinical malaria incidence at a fine scale in a cohort of children under five in an endemic area in rural Chikhwawa, Malawi, determined associated factors, and monitored adult mosquito abundance.
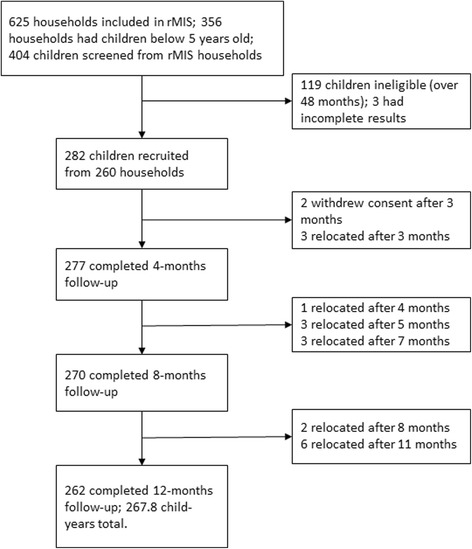
Methods: We followed-up 285 children aged 6-48 months with recorded geolocations, who were sampled in a rolling malaria indicator survey, for one year (2015-2016). Guardians were requested to take the children to a nearby health facility whenever ill, where health facility personnel were trained to record malaria test results and temperature on the child's sick-visit card; artemisinin-based combination therapy was provided if indicated. The cards were collected and replaced 2-monthly. Adult mosquitoes were collected from 2-monthly household surveys using a Suna trap. The head/thorax of adult Anopheles females were tested for presence of Plasmodium DNA. Binomial logistic regression and geospatial modelling were performed to determine predictors of and to spatially predict clinical malaria incidence, respectively.
Results: Two hundred eighty two children, with complete results, and 267.8 child-years follow-up time were included in the analysis. The incidence rate of clinical malaria was 1.2 cases per child-year at risk; 57.1% of the children had at least one clinical malaria case during follow-up. Geographical groups of households where children experienced repeated malaria infections overlapped with high mosquito densities and high entomological inoculation rate locations.
Conclusions: Repeated malaria infections within household groups account for the majority of cases and signify uneven distribution of malaria risk within a small geographical area.
Keywords: Entomological surveillance; Incidence rate; Malaria; Spatio-temporal heterogeneity.
Conflict of interest statement
Ethics approval and consent to participate
Both studies were reviewed and approved by College of Medicine Research Ethics Committee (P.11/14/1658, P.09/14/1631). An informed consent was obtained from study participants’ guardians.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures



References
-
- Staedke SG, Nottingham EW, Cox J, Kamya MR, Rosenthal PJ, Dorsey G. Short report: proximity to mosquito breeding sites as a risk factor for clinical malaria episodes in an urban cohort of Ugandan children. Am J Trop Med Hyg. 2003;69:244–246. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
