

Association of Nonoxidized Parathyroid Hormone with Cardiovascular and Kidney Disease Outcomes in Chronic Kidney Disease
- PMID: 29507005
- PMCID: PMC5968904
- DOI: 10.2215/CJN.06620617
Association of Nonoxidized Parathyroid Hormone with Cardiovascular and Kidney Disease Outcomes in Chronic Kidney Disease
Abstract
Background and objectives: In patients with CKD, elevated plasma parathyroid hormone (PTH) levels are associated with greater cardiovascular morbidity and mortality. However, the reference method for PTH measurement is disputed. It has been argued that measurement of nonoxidized PTH better reflects biologically active PTH than measurements with conventional assays.
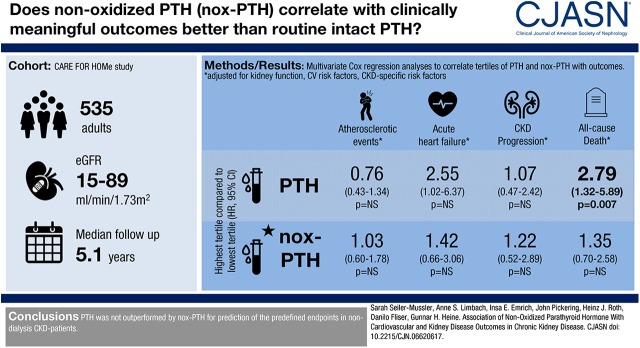
Design, setting, participants, & measurements: PTH and nonoxidized PTH levels were measured at study baseline in 535 patients with CKD with an eGFR range between 89 and 15 ml/min per 1.73 m2. Patients were followed over 5.1 years for the occurrence of acute heart failure, atherosclerotic events, CKD progression (doubling of serum creatinine or initiation of RRT), or all-cause death.
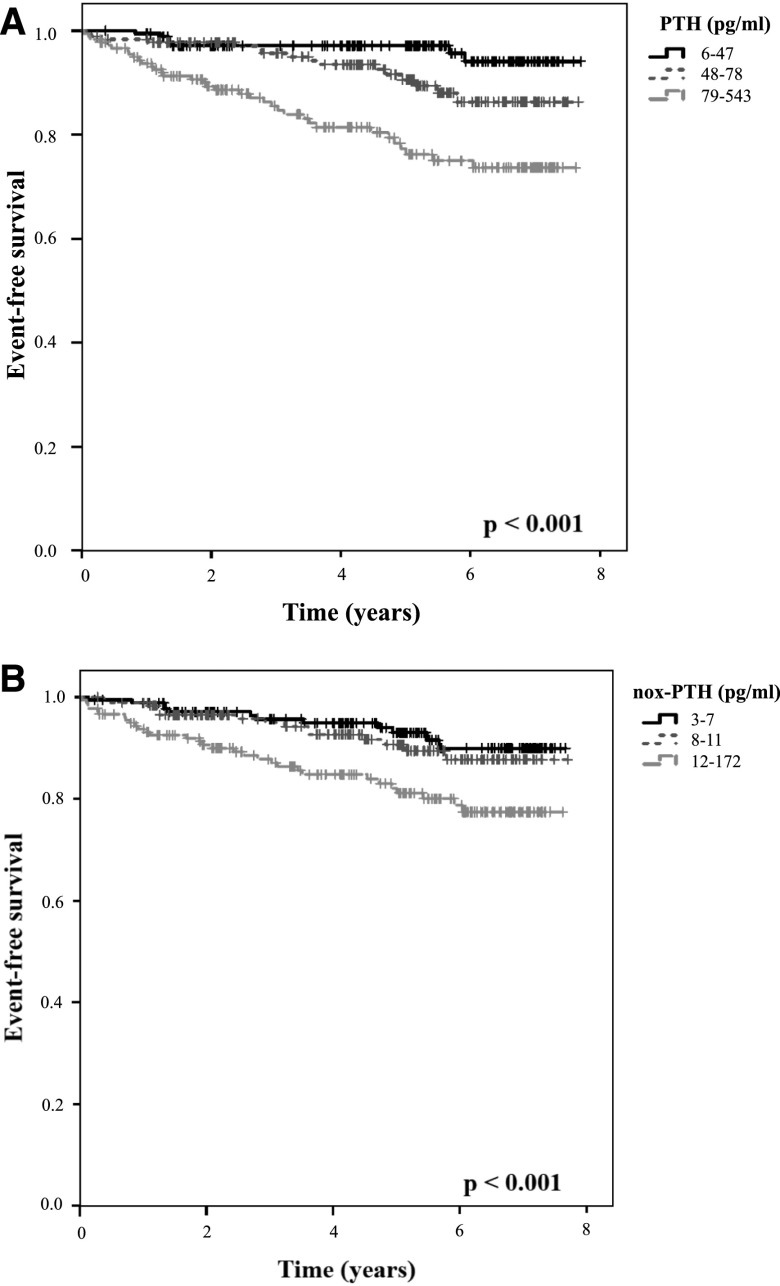
Results: Atherosclerotic events, acute heart failure, CKD progression, and deaths from any cause occurred in 116, 58, 73, and 85 patients, respectively. In Kaplan-Meier analyses, patients at the highest PTH and nonoxidized-PTH tertile (79-543 and 12-172 pg/ml, respectively) showed a higher rate of atherosclerotic events, acute heart failure, CKD progression, and death from any cause. After adjustment for eGFR and albuminuria, nonoxidized PTH was no longer associated with atherosclerotic events (hazard ratio third versus first tertile, 1.04 [95% confidence intervals, 0.62-1.75]), acute heart failure (hazard ratio third versus first tertile, 1.24 [95% confidence intervals, 0.59-2.62]), CKD progression (hazard ratio third versus first tertile, 0.93 [95% confidence intervals, 0.46-1.90]), and death from any cause (hazard ratio third versus first tertile, 1.23 [95% confidence intervals, 0.66-2.31]), and PTH lost its association with atherosclerotic events (hazard ratio third versus first tertile, 0.80 [95% confidence intervals, 0.46-1.38]) and CKD progression (hazard ratio third versus first tertile, 0.99 [95% confidence intervals, 0.46-2.10]), although it remained associated with acute heart failure (hazard ratio third versus first tertile, 2.76 [95% confidence intervals, 1.11-6.89]) and all-cause death (hazard ratio third versus first tertile, 2.35 [95% confidence intervals, 1.13-4.89]). After further adjustment for cardiovascular and kidney risk factors, PTH remained associated with all-cause death (hazard ratio third versus first tertile, 2.79 [95% confidence intervals, 1.32-5.89]), but with no other end point.
Conclusions: In a cohort of patients with CKD, PTH was associated with all-cause mortality; there was no association of nonoxidized PTH with any of the clinical outcomes examined.
Keywords: Cause of Death; Disease Progression; Humans; Renal Insufficiency, Chronic; Renal Replacement Therapy; albuminuria; cardiovascular disease; chronic kidney disease; clinical epidemiology; creatinine; heart failure; kidney; parathyroid hormone; risk factors.
Copyright © 2018 by the American Society of Nephrology.
Figures
Comment in
-
Clear the Fog around Parathyroid Hormone Assays: What Do iPTH Assays Really Measure?Clin J Am Soc Nephrol. 2018 Apr 6;13(4):524-526. doi: 10.2215/CJN.01730218. Epub 2018 Mar 5. Clin J Am Soc Nephrol. 2018. PMID: 29507007 Free PMC article. No abstract available.
References
-
- Foley RN, Parfrey PS: Cardiovascular disease and mortality in ESRD. J Nephrol 11: 239–245, 1998 - PubMed
-
- Foley RN, Parfrey PS, Harnett JD, Kent GM, O’Dea R, Murray DC, Barre PE: Mode of dialysis therapy and mortality in end-stage renal disease. J Am Soc Nephrol 9: 267–276, 1998 - PubMed
-
- de Jager DJ, Grootendorst DC, Jager KJ, van Dijk PC, Tomas LM, Ansell D, Collart F, Finne P, Heaf JG, De Meester J, Wetzels JF, Rosendaal FR, Dekker FW: Cardiovascular and noncardiovascular mortality among patients starting dialysis. JAMA 302: 1782–1789, 2009 - PubMed
-
- Herzog CA, Asinger RW, Berger AK, Charytan DM, Díez J, Hart RG, Eckardt KU, Kasiske BL, McCullough PA, Passman RS, DeLoach SS, Pun PH, Ritz E: Cardiovascular disease in chronic kidney disease. A clinical update from Kidney Disease: Improving Global Outcomes (KDIGO). Kidney Int 80: 572–586, 2011 - PubMed
-
- Ketteler M, Block GA, Evenepoel P, Fukagawa M, Herzog CA, McCann L, Moe SM, Shroff R, Tonelli MA, Toussaint ND, Vervloet MG, Leonard MB: Executive summary of the 2017 KDIGO Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) guideline update: What’s changed and why it matters. Kidney Int 92: 26–36, 2017 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
