

Eyes and stroke: the visual aspects of cerebrovascular disease
- PMID: 29507782
- PMCID: PMC5829892
- DOI: 10.1136/svn-2017-000079
Eyes and stroke: the visual aspects of cerebrovascular disease
Abstract
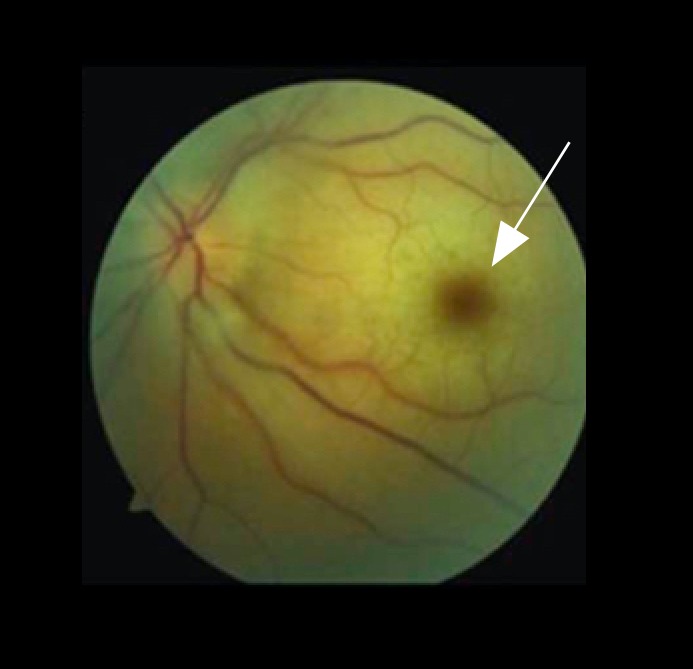
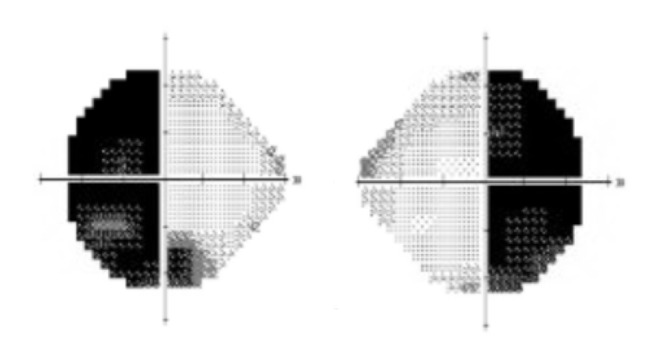
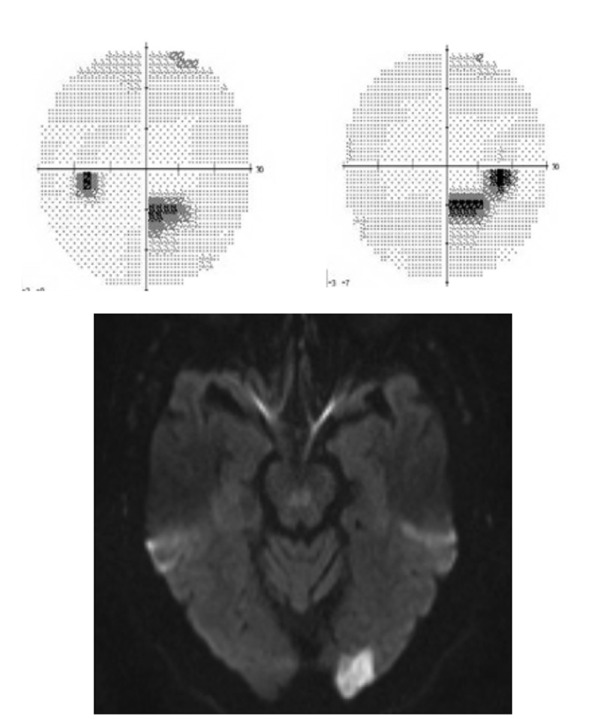
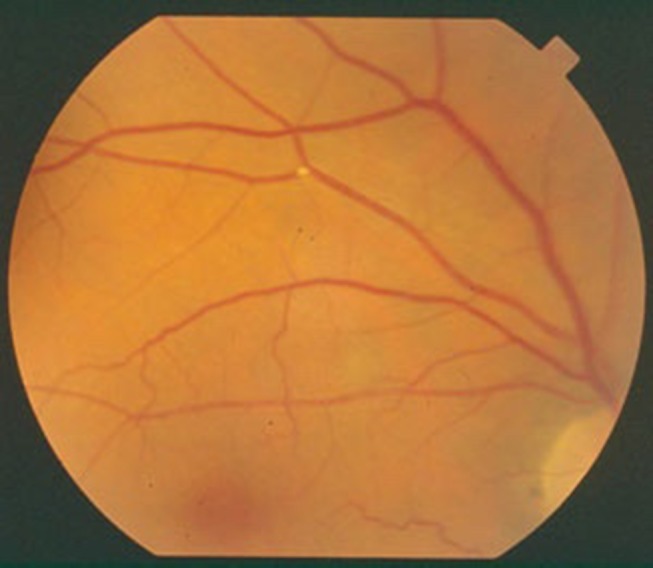
A large portion of the central nervous system is dedicated to vision and therefore strokes have a high likelihood of involving vision in some way. Vision loss can be the most disabling residual effect after a cerebral infarction. Transient vision problems can likewise be a harbinger of stroke and prompt evaluation after recognition of visual symptoms can prevent future vascular injury. In this review, we discuss the visual aspects of stroke. First, anatomy and the vascular supply of the visual system are considered. Then, the different stroke syndromes which involve vision are discussed. Finally, topics involving the assessment, prognosis, treatment and therapeutic intervention of vision-specific stroke topics are reviewed.
Keywords: Amaurosis Fugax; Diplopia; Homonymous hemianopia; Stroke; Vision.
Conflict of interest statement
Competing interests: None declared.
Figures


References
-
- Rowe FJ, Wright D, Brand D, et al. A prospective profile of visual field loss following stroke: prevalence, type, rehabilitation, and outcome. Biomed Res Int 2013;2013:1–12. (719096) doi:10.1155/2013/719096 - DOI - PMC - PubMed
-
- Sand KM, Wilhelmsen G, Naess H, et al. Vision problems in ischaemic stroke patients: effects on life quality and disability. Eur J Neurol 2016;23:1–7. doi:10.1111/ene.12848 - DOI - PubMed
-
- Varma DD, Cugati S, Lee AW, et al. A review of central retinal artery occlusion: clinical presentation and management. Eye 2013;27:688–97. doi:10.1038/eye.2013.25 - DOI - PMC - PubMed
-
- de Vries TM, Aries MJ, De Groot JC, et al. A grid-like hemi-field defect following a lacunar infarct in the lateral geniculate nucleus. Clin Neurol Neurosurg 2012;114:278–80. doi:10.1016/j.clineuro.2011.10.021 - DOI - PubMed
-
- Tsuda H, Yoshizawa T. Localized infarction of the lateral geniculate body. Intern Med 2014;53:1891–2. doi:10.2169/internalmedicine.53.2695 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical