

Association of Severity of Coronary Artery Aneurysms in Patients With Kawasaki Disease and Risk of Later Coronary Events
- PMID: 29507955
- PMCID: PMC5875323
- DOI: 10.1001/jamapediatrics.2018.0030
Association of Severity of Coronary Artery Aneurysms in Patients With Kawasaki Disease and Risk of Later Coronary Events
Abstract
Importance: Few studies with sufficient statistical power have shown the association of the z score of the coronary arterial internal diameter with coronary events (CE) in patients with Kawasaki disease (KD) with coronary artery aneurysms (CAA).
Objective: To clarify the association of the z score with time-dependent CE occurrence in patients with KD with CAA.
Design, setting, and participants: This multicenter, collaborative retrospective cohort study of 44 participating institutions included 1006 patients with KD younger than 19 years who received a coronary angiography between 1992 and 2011.
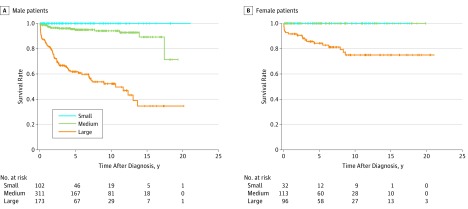
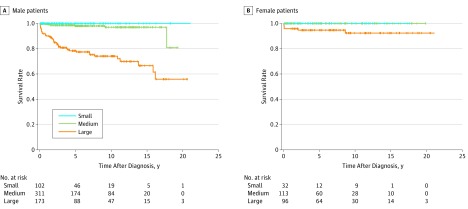
Main outcomes and measures: The time-dependent occurrence of CE, including thrombosis, stenosis, obstruction, acute ischemic events, and coronary interventions, was analyzed for small (z score, <5), medium (z score, ≥5 to <10; actual internal diameter, <8 mm), and large (z score, ≥10 or ≥8 mm) CAA by the Kaplan-Meier method. The Cox proportional hazard regression model was used to identify risk factors for CE after adjusting for age, sex, size, morphology, number of CAA, resistance to initial intravenous immunoglobulin (IVIG) therapy, and antithrombotic medications.
Results: Of 1006 patients, 714 (71%) were male, 341 (34%) received a diagnosis before age 1 year, 501 (50%) received a diagnosis between age 1 and 5 years, and 157 (16%) received a diagnosis at age 5 years or older. The 10-year event-free survival rate for CE was 100%, 94%, and 52% in men (P < .001) and 100%, 100%, and 75% in women (P < .001) for small, medium, and large CAA, respectively. The CE-free rate was 100%, 96%, and 79% in patients who were not resistant to IVIG therapy (P < .001) and 100%, 96%, and 51% in patients who were resistant to IVIG therapy (P < .001), respectively. Cox regression analysis revealed that large CAA (hazard ratio, 8.9; 95% CI, 5.1-15.4), male sex (hazard ratio, 2.8; 95% CI, 1.7-4.8), and resistance to IVIG therapy (hazard ratio, 2.2; 95% CI, 1.4-3.6) were significantly associated with CE.
Conclusions and relevance: Classification using the internal diameter z score is useful for assessing the severity of CAA in relation to the time-dependent occurrence of CE and associated factors in patients with KD. Careful management of CE is necessary for all patients with KD with CAA, especially men and IVIG-resistant patients with a large CAA.
Conflict of interest statement
Figures
References
-
- Ogawa S, Ayusawa M, Fukazawa R, et al. ; JCS Joint Working Group . Guidelines for diagnosis and management of cardiovascular sequelae in Kawasaki disease (JCS 2013). Digest version. Circ J. 2014;78(10):-. - PubMed
-
- Manlhiot C, Millar K, Golding F, McCrindle BW. Improved classification of coronary artery abnormalities based only on coronary artery z-scores after Kawasaki disease. Pediatr Cardiol. 2010;31(2):242-249. - PubMed
-
- McCrindle BW, Rowley AH, Newburger JW, et al. ; American Heart Association Rheumatic Fever, Endocarditis, and Kawasaki Disease Committee of the Council on Cardiovascular Disease in the Young; Council on Cardiovascular and Stroke Nursing; Council on Cardiovascular Surgery and Anesthesia; and Council on Epidemiology and Prevention . Diagnosis, treatment, and long-term management of Kawasaki disease: a scientific statement for health professionals from the American Heart Association. Circulation. 2017;135(17):e927-e999. - PubMed
-
- de Zorzi A, Colan SD, Gauvreau K, Baker AL, Sundel RP, Newburger JW. Coronary artery dimensions may be misclassified as normal in Kawasaki disease. J Pediatr. 1998;133(2):254-258. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
